[level-membership-for-dermatology-category]
Bacterial infection – Staphylococcal and streptococcal
The skin is a barrier to infection but, if its defences are penetrated or broken down, numerous micro-organisms can cause disease (Table 1).
Table 1 Bacterial diseases of the skin
| Organism | Infection |
|---|---|
| Commensals | Erythrasma, pitted keratolysis, trichomycosis axillaris |
| Staphylococci | Impetigo, ecthyma, folliculitis, secondary infection |
| Streptococci | Erysipelas, cellulitis, impetigo, ecthyma, necrotizing fasciitis |
| Gram-negative | Secondary infection, folliculitis, cellulitis |
| Mycobacterial | TB (lupus vulgaris, warty tuberculosis, scrofuloderma), fish tank granuloma, Buruli ulcer, leprosy |
| Spirochaetes | Syphilis (e.g. primary, secondary), Lyme disease (erythema chronicum migrans) |
| Neisseria | Gonorrhoea (pustules), meningococcaemia (purpura) |
| Others | Anthrax (pustule), erysipeloid (pustule) |
Staphylococcal infections
Impetigo
Clinical presentation
Impetigo is now relatively uncommon in the UK, mainly because of improved social conditions, but it is endemic in developing countries. It generally occurs in children and presents as thin-walled, easily ruptured vesicles, often on the face, which leave areas of yellow-crusted exudate (Fig. 1). Lesions spread rapidly and are contagious. A bullous form, with blisters 1–2 cm in diameter, is seen in all ages and affects the face or extremities. Atopic eczema, scabies, herpes simplex and lice infestation may all become impetiginized. Impetigo can be confused with herpes simplex or a fungal infection.

Ecthyma
Ecthyma is characterized by circumscribed, ulcerated and crusted infected lesions that heal with scarring. An insect bite or neglected minor injury may become infected with staphylococci or streptococci (or both). Ecthyma mostly occurs on the legs (Fig. 2) and may be seen in drug addicts or debilitated patients. Treatment is with systemic and topical antibiotics.

Folliculitis and related conditions
Clinical presentation
Follicular pustules are seen in hair-bearing areas, e.g. the legs, scalp or face. In men, folliculitis may affect the beard area (sycosis barbae). In women, it may occur on the legs after hair removal by shaving or waxing. Staph. aureus is usually, but not invariably, responsible. Strains carrying the virulence factor Panton–Valentine leukocidin (PVL) are associated with more aggressive disease. A Gram-negative folliculitis (e.g. with Pseudomonas) may occur with prolonged antibiotic treatment for acne. Pityrosporum folliculitis is a separate condition due to a commensal yeast (p. 38).
Furuncles (boils) present as tender red pustules that suppurate and heal with scarring. They often occur on the face, neck, scalp, axillae and perineum. Some patients have recurrent staphylococcal boils of the axillae or perineum. Large suppurating carbuncles (Fig. 3) due to Staph. aureus may cause systemic upset.

Staphylococcal scalded skin syndrome
Staphylococcal scalded skin syndrome is an acute toxic illness, usually of infants, in which there is shedding of sheets of epidermis associated with localized staphylococcal infection in the skin or elsewhere. Large sheets of superficial epidermis are shed, resembling a scald, leaving denuded erythematous areas. Phage group II staphylococci release into the bloodstream epidermolytic toxins, which cause the epidermis to split. A related condition in adults with the same level of epidermal split is pemphigus foliaceus (p. 87).
Streptococcal infections
Erysipelas
Clinical presentation
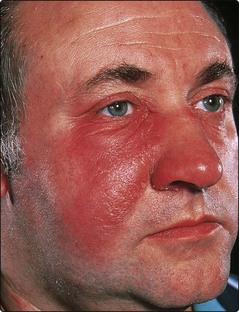
The skin lesions may be preceded by fever, malaise and ‘flu-like’ symptoms. Erysipelas usually affects the face (where it may be bilateral) or the lower leg, and appears as a painful hot red swelling (Fig. 4). The lesion has a well-defined edge and may blister. Cellulitis may coexist. The streptococci usually gain entry to the skin via a fissure, e.g. behind the ear, or associated with tinea pedis between the toes.
Differential diagnosis and complications
On the face, erysipelas may be confused with angioedema or allergic contact dermatitis, but the condition is usually distinguishable as it causes tenderness and systemic upset. Recurrent attacks in the same place can result in lymphoedema due to lymphatic damage. A fatal streptococcal septicaemia can occur in debilitated patients. Guttate psoriasis (p. 28) and acute glomerulonephritis may follow a streptococcal infection.




[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Bacterial infection – Staphylococcal and streptococcal
The skin is a barrier to infection but, if its defences are penetrated or broken down, numerous micro-organisms can cause disease (Table 1).
Table 1 Bacterial diseases of the skin
| Organism | Infection |
|---|---|
| Commensals | Erythrasma, pitted keratolysis, trichomycosis axillaris |
| Staphylococci | Impetigo, ecthyma, folliculitis, secondary infection |
| Streptococci | Erysipelas, cellulitis, impetigo, ecthyma, necrotizing fasciitis |
| Gram-negative | Secondary infection, folliculitis, cellulitis |
| Mycobacterial | TB (lupus vulgaris, warty tuberculosis, scrofuloderma), fish tank granuloma, Buruli ulcer, leprosy |
| Spirochaetes | Syphilis (e.g. primary, secondary), Lyme disease (erythema chronicum migrans) |
| Neisseria | Gonorrhoea (pustules), meningococcaemia (purpura) |
| Others | Anthrax (pustule), erysipeloid (pustule) |
Staphylococcal infections
Impetigo
Clinical presentation
Impetigo is now relatively uncommon in the UK, mainly because of improved social conditions, but it is endemic in developing countries. It generally occurs in children and presents as thin-walled, easily ruptured vesicles, often on the face, which leave areas of yellow-crusted exudate (Fig. 1). Lesions spread rapidly and are contagious. A bullous form, with blisters 1–2 cm in diameter, is seen in all ages and affects the face or extremities. Atopic eczema, scabies, herpes simplex and lice infestation may all become impetiginized. Impetigo can be confused with herpes simplex or a fungal infection.
[/not-level-membership-for-dermatology-category]
