Chapter 20 Axial magnetic resonance imaging
Internal neural relations
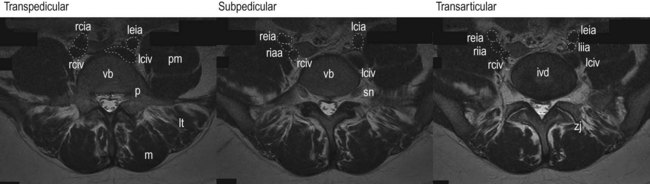
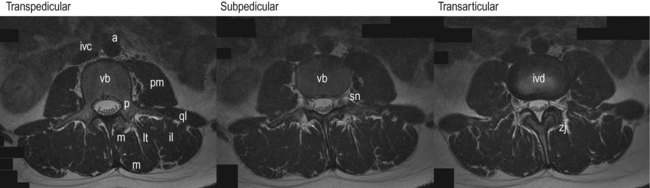
Axial magnetic resonance imaging (MRI) scans of the lumbar spine are typical taken through three standard locations at any given segment. The scans can be through the pedicles (transpedicular), below the pedicles (subpedicular) or through the intervertebral disc and zygapophysial joints (transarticular) (Fig. 20.1).

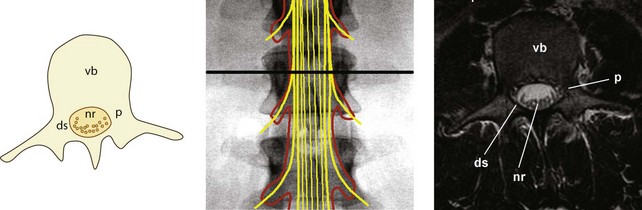
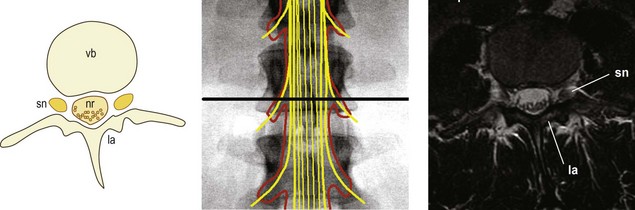
Each of these scans intersects slightly different elements contained within the vertebral canal. Transpedicular scans will intersect the dural sac and the nerve roots of the cauda equina (Fig. 20.2). In these scans, the pedicles will be evident projecting from the posterior surface of the vertebral body. These bones present as a grey signal. Posteriorly, various parts of the laminae and spinous process will complete the vertebral canal. Within the vertebral canal, the dural sac will appear as a black circle or oval, enclosing a white signal generated by the cerebrospinal fluid within the sac. Inside the sac, the nerve roots of the cauda equina appear as block dots, because the nerves appear as if they have been transected and looked at end-on. The nerve roots typically appear towards the posterior surface of the dural sac because patients typically lie supine when the scan is taken, and the nerve roots ‘fall’ to the rear.
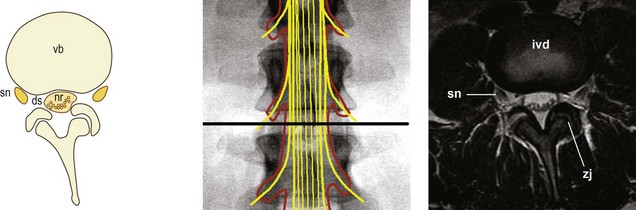
Subpedicular scans will intersect the nerve roots of the cauda equina but also the spinal nerves of the segment, as they run through the intervertebral foramen of the segment (Fig. 20.3). The scan will show the vertebral body anteriorly, and the lamina on each side posteriorly. Behind the centre of the vertebral body, the dural sac will appear as a dark ring, with the nerve roots of the cauda equina appearing as black dots lying in a sea of white signal formed by the cerebrospinal fluid. Lateral to the dural sac a dark signal will appear, behind the vertebral body, created by the spinal nerve. Depending on exactly where the scan is taken, the spinal nerve may be accompanied by a sleeve of dura mater, which in turn may contain a sliver of cerebrospinal fluid surrounding the nerve.
Transarticular scans will intersect the dural sac and cauda equina centrally, but will also show the spinal nerve or ventral ramus leaving the vertebral column and entering the psoas major muscle (Fig. 20.4). Anteriorly, the scan will show the intervertebral disc. Unlike the vertebral body, which appeared grey, the disc will largely appear black. The centre of the disc may appear grey if the scan is taken close to the vertebral endplate. Posteriorly, the zygapophysial joints will be evident. Centrally, the dural sac will enclose the nerve roots of the cauda equina, as in transpedicular scans. Laterally, near the posterolateral corner of the disc, a dark rounded signal is produced by the spinal nerve becoming the ventral ramus. Because the spinal nerve passes obliquely and caudally through the intervertebral foramen, it will be located further laterally, i.e. peripherally, in transarticular scans than in subpedicular scans, and will be distinctly dissociated from the dural sac.
External relations
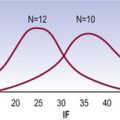
The external relations that will be seen on an axial scan will differ at different segmental levels. Figure 20.5 summarises what structure the reader should expect at different segments, and what each structure should look like.
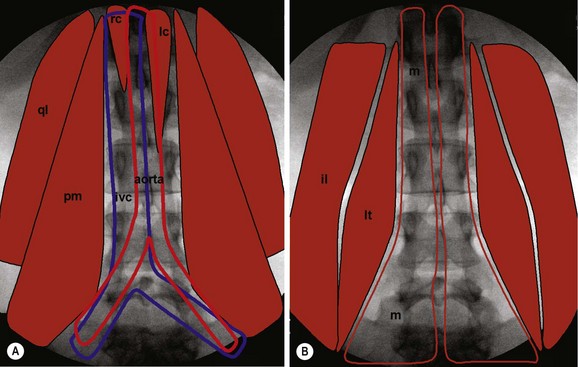
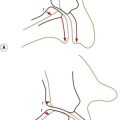
At upper lumbar levels, the reader should expect to encounter the left crus and right crus of the diaphragm, arising from the front of the vertebral bodies (Fig. 20.5A). In particular, the crura will be large in front of L1 but tapering and dissipating in front of L2. The crura intervene between the vertebral column and the inferior vena cava and the aorta.
The inferior vena cava lies to the right, and the reader should expect to encounter it at all segmental levels as far as L5 (Fig. 20.5A). The aorta lies towards the midline at upper lumbar levels, but deviates somewhat to the left, until it divides at L4 (Fig. 20.5A). At the L1, L2 and L3 levels, the reader should expect to encounter two large vessels: the inferior vena cava and the aorta. At L4, the reader should expect to encounter three vessels: the inferior vena cava and the aorta having divided into the two common iliac arteries. At L5, the reader should expect four vessels: the two common iliac arteries and the two common iliac veins. The number of great vessels in front the vertebra column is the most obvious indication of whether the scan is at L5 or at L4, or at L1, 2 or 3.
Laterally, the reader should expect to encounter quadratus lumborum as a broad, flat mass overlying the transverse processes (Fig. 20.5A); but not at L5, for the quadratus lumborum arises from the iliolumbar ligament and, therefore, above L5. The absence of quadratus lumborum is one of the features that characterise scans at L5.
The psoas major covers the quadratus lumborum, but progressively enlarges from L1 to L5 (Fig. 20.5A). Therefore, in axial scans, the reader should expect psoas to be narrow at upper lumbar levels, and progressively thicker at lower levels. Indeed, compared to other structures, psoas becomes enormous at lower lumbar levels.
Posteriorly, the reader should expect to encounter the three major posterior back muscles. They should expect multifidus to be confined to the region over the lamina at upper lumbar levels, but to expand progressively widely from L3 to the sacrum (Fig. 20.5B). Lateral to multifidus, the reader should expect the longissimus thoracis to be centred over the roots of the transverse processes; and the iliocostalis lumborum to be centred over the tips of the transverse processes.
Axial MRI scans at L1
Using Figure 20.5, the reader should expect to encounter the left crus and right crus in scans at L1, with the inferior vena cava and aorta in front of them. Lateral to the vertebral bodies, the reader should expect a broad, flat quadratus lumborum, but a narrow psoas major, for its fibres will have just arisen from the T12–L1 disc. Posteriorly, the reader should expect a narrow multifidus, flanked by longissimus thoracis and iliocostalis lumborum. This is indeed what scans through L1 show (Fig. 20.6).

Axial MRI scans at L2
Using Figure 20.5, the reader should expect modifications at scans through L2. The crura will be attenuated, but the inferior vena cava and aorta will be prominent, anteriorly. The quadratus lumborum should persist, but the psoas major should be larger. Posteriorly, the multifidus, longissimus thoracis, and iliocostalis lumborum should be evident. This is indeed what scans through L2 show (Fig. 20.7).

Scans through L1 and L2 may be quite similar, and may be difficult to distinguish. The immediate differences are only relative: the crura are small, or absent, at L2; and the psoas is only relatively larger. On these grounds alone, readers could be excused for not being able to distinguish absolutely scans through L1 and L2. Further clues appear in the visceral and vascular structures lying anterior to the lumbar spine. For example, the right renal vessels tend to be more caudal than those on the left. Therefore, left renal vessels are likely to be encountered at L1, whereas right renal vessels will be seen at L2 (Fig. 20.7). The anatomy of visceral and vascular structures, however, is outside the scope of this text.
Axial MRI scans at L3
Using Figure 20.5, the reader should expect no crura in scans at L3, but the inferior vena cava and aorta will be prominent, anterior to the vertebral column. The quadratus lumborum should be evident, and the psoas major should appear as a substantial mass. Posteriorly, the multifidus should be expanding lateral to the limits of the laminae; but otherwise, it will be flanked by the longissimus thoracis and the iliocostalis lumborum. This is indeed what scans through L3 show (Fig. 20.8). The absence of crura, the prominence of psoas and the expansion of multifidus all characterise scans through L3.
Axial MRI scans at L4
Using Figure 20.5, the reader should expect to see three great vessels in front of the vertebral column in scans through L4. Laterally, the psoas should be large. Posteriorly, the multifidus should be wide, and the erector spinae should be correspondingly small. This is indeed what scans through L4 show (Fig. 20.9).

Axial MRI scans at L5
Using Figure 20.5, the reader should expect to see four great vessels in front of the vertebral column in scans through L5. Laterally, the psoas should be huge, but the quadratus lumborum should be absent. If the scan passes through the appropriate level, the iliolumbar ligament might be evident. Posteriorly, the multifidus will be very wide. The iliocostalis will be lacking, because its insertion – into the iliac crest – lies above L5. Only a small portion of longissimus thoracis should be evident. This is indeed what scans through L5 show (Fig. 20.10).