[level-membership-for-radiology-category] Free-flowing ascites conforms to shape of surrounding structures and flows to dependent recesses
Simple fluid signal on T1WI (hypointense) and T2WI (hyperintense) MR
No appreciable complexity within ascites fluid
• Exudative ascites: Typically demonstrates increasing density of fluid with increasing protein content
Often mildly hyperdense (15-30 HU) relative to transudative ascites
May demonstrate complexity, including septations, peritoneal thickening/enhancement, and loculation
Loculated ascites fluid exerts mass effect and displaces adjacent structures (such as bowel loops)
Usually simple fluid signal on T1WI and T2WI MR, but internal complexity and protein can result in intermediate T1 and T2 signal
Chylous ascites can measure < 0 HU or demonstrate fat-fluid levels
PATHOLOGY
• Ascites is typically divided into 2 types
Transudative ascites is caused by high portal venous pressures and is characterized by low protein, low LDH, normal glucose, and low specific gravity
– Transudative ascites is simple ascites fluid most often caused by cirrhosis, hepatitis, heart failure, renal failure, hypoproteinemia, etc.
Exudative ascites is characterized by high protein and high specific gravity
– Exudative ascites related to multiple causes, such as infection, ischemia, peritoneal carcinomatosis, peritonitis, or pancreatitis
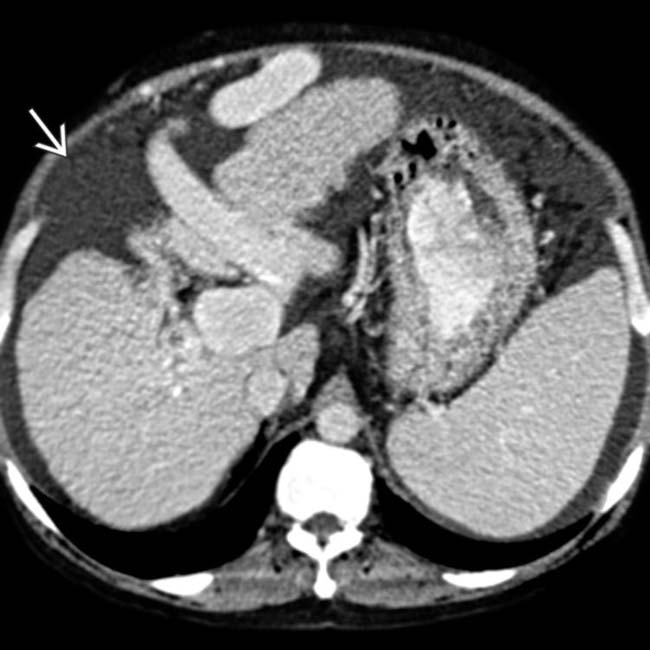
(Left) Axial CECT shows ascites due to hepatic cirrhosis, with large varices and splenomegaly. Notice the relatively simple, uncomplicated appearance of this transudative ascites.
(Right) Axial CECT shows massive ascites due to right heart failure. Like other forms of transudative ascites, note that the fluid appears simple without evidence of complexity, nodularity, or adjacent peritoneal thickening/enhancement.
(Left) Ultrasound shows large anechoic ascites in the lower abdomen displacing bowel loops in a patient with cirrhosis. As in this case, simple transudative ascites is classically anechoic, freely mobile, and shows acoustic enhancement.
(Right) Ultrasound shows complicated ascites in a cirrhotic patient. The fluid was non-mobile and loculated on real-time scanning, and there are multiple internal septations , suggesting this is not simple transudative ascites. The ascites fluid was found to be infected.
TERMINOLOGY
Definitions
• Pathologic accumulation of fluid within peritoneal cavity
IMAGING
General Features
• Best diagnostic clue
Diagnostic paracentesis (in cases where either infection or tumor is suspected)
• Location
Free-flowing ascites fluid flows to most dependent recesses of abdomen and pelvis
– Morison pouch (hepatorenal fossa): Most dependent recess in upper abdomen
– Rectouterine or rectovesical space: Most dependent spaces in pelvis
– Paracolic gutters and subphrenic spaces
– Lesser sac usually does not fill with ascites, with the exception of cases with tense ascites or ascites due to a local source (gastric ulcer or pancreatitis)
Otherwise, lesser sac fluid suspicious for ascites related to carcinomatosis or infection
• Morphology
Free-flowing ascites: Conforms to shape of surrounding structures and does not deform normal shape of adjacent organs or exert mass effect
– Fluid insinuates itself between organs
Loculated fluid: Fluid demonstrates rounded contour and appears encapsulated
– Loculated ascites fluid exerts mass effect and displaces adjacent structures (such as bowel loops)
• Key concepts and descriptors
Ascites typically divided into 2 types
– Transudative ascites is caused by high portal venous pressures and is characterized by low protein, low LDH, normal glucose, and low specific gravity
Transudative ascites is simple ascites fluid that is most often caused by cirrhosis, hepatitis, heart failure, renal failure, or hypoproteinemia
– Exudative ascites characterized by high protein and high specific gravity
Exudative ascites related to multiple causes, such as infection, ischemia, peritoneal carcinomatosis, peritonitis, and pancreatitis
• Abdominal radiograph: Insensitive for fluid, as diagnosis of ascites on radiographs requires a substantial amount of fluid to be present (usually > 500 cc)
Diffuse haziness and increased density of abdomen
Poor visualization of normally visualized soft tissue structures, such as psoas and renal outline
– Obliteration of hepatic and splenic angles
Bulging of flanks due to fluid distending abdomen
Separation of small bowel loops with centralization of floating gas-containing small bowel
Hellmer sign: Lateral edge of liver medially displaced from adjacent thoracoabdominal wall
Symmetric densities on sides of bladder (dog ears sign)
Medial displacement of ascending and descending colon
Lateral displacement of properitoneal fat line
CT Findings
• Transudative ascites
Typical transudative ascites has density of 0-15 Hounsfield units (HU) and appears free flowing
Small amounts of ascites typically seen in right perihepatic space, Morison pouch, and pouch of Douglas
Larger amounts of fluid accumulate in paracolic gutters
– Ascites can cause centralization of bowel loops
– Ascites accumulating in central abdomen may have triangular configuration within leaves of mesentery
Massive ascites distends peritoneal spaces
Look for associated evidence of liver, heart, or kidney failure (most common causes of transudative ascites)
• Exudative ascites
Exudative ascites typically demonstrates increasing density of fluid with increasing protein content
– Exudative ascites often mildly hyperdense relative to transudative ascites (15-30 HU)
– May demonstrate complexity, including septations, peritoneal thickening/enhancement, and loculation
Ascites related to peritoneal carcinomatosis: Complex ascites with nodularity and thickening of adjacent peritoneum and frequent loculation of ascites
Chylous ascites: Intraperitoneal and extraperitoneal fluid usually of water density, but can be < 0 HU or demonstrate fat-fluid levels (due to fat content)
Bile ascites: Low density fluid (usually < 15 HU) most typically localized adjacent to liver or biliary structures
– Bilomas (loculated collections of bile fluid) sharp margins
Urinary ascites: Low density fluid (< 15 HU) usually localized adjacent to urinary tract (and site of leak)
– IV contrast accumulates within ascites fluid during excretory phase (after renal concentration and excretion)
Cerebrospinal fluid ascites: Small amount of free fluid is expected with ventriculoperitoneal shunt
– Localized collection near tip of shunt catheter is abnormal and implies malfunction
Pancreatic ascites: Most often accumulates surrounding pancreas, lesser sac, and anterior pararenal space
– Usually seen in presence of severe pancreatitis or disruption of pancreatic duct
Pseudomyxoma peritonei: Large low-attenuation collection, multiseptate, loculations
– Multiple cystic-appearing masses, calcification
– Thickening of peritoneal and omental surface
– Scalloping of liver and spleen contour
MR Findings
• Transudative ascites: Fluid signal on T1WI (hypointense) and T2WI (hyperintense)
• Exudative: Usually simple fluid signal on T1WI and T2WI, but internal complexity and protein can result in intermediate T1 and T2 signal
Internal complexity (such as debris or septations) usually more apparent on MR compared to CT
• Artifacts
Flow voids related to bulk motion of fluid usually more evident on SSFSE/HASTE sequences (compared to T2 FSE or steady state free precession/SSFP) and should not be misinterpreted as tumor or carcinomatosis
Failure of fat suppression adjacent to sites of susceptibility (i.e., gas within bowel) can be misinterpreted as ascites fluid
– Ascites often erroneously diagnosed near diaphragm due to susceptibility from adjacent lung
Ultrasonographic Findings
• Uncomplicated ascites
Homogeneous, freely mobile, anechoic fluid with posterior acoustic through transmission
Free fluid forms acute angles where fluid borders organs, should shift with changes in patient position, and should compress with increased transducer pressure
Polycyclic, lollipop, arcuate appearance: Small bowel loops arrayed on either side of vertically floating mesentery in patients with massive ascites
Transverse and sigmoid colon usually float on top of fluid (nondependent gas content when patient is supine)
• Complicated exudative ascites
May demonstrate internal echoes or septations
– Blood often produces coarse echoes and chyle produces fine echoes
Fluid is often loculated (i.e., not freely mobile with changes in position or transducer compression)
– Loculated ascites implies adhesions, malignancy, or infection of peritoneum
Internal septations more apparent on US than CT
– Matted or clumped, infiltrated bowel loops
– Thickened interfaces between fluid and adjacent structures, peritoneal lining, omental thickening
• Thickening of gall bladder wall, > 3 mm in benign ascites, < 3 mm in carcinomatosis
• Sonolucent band; small amounts of fluid in Morison pouch, around liver
Imaging Recommendations
• US: Simple, cost-effective, and very sensitive (can detect volumes of ascites as small as 5-10 mL)
• CT: Valuable for evaluating underlying cause of ascites
DIFFERENTIAL DIAGNOSIS
Hemoperitoneum
• High-attenuation fluid which is typically > 30 HU (30-60 HU), although will gradually decrease in density over time
Active hemorrhage results in fluid at site of extravasation which is isodense to contrast-enhanced blood vessels
Sentinel clot: Highest density (> 60 HU) blood products accumulate near site of bleeding
Malignant Ascites
• Exudative ascites which is often loculated and associated with nodular thickening of peritoneum and carcinomatosis
• Known underlying malignancy and imaging evidence of metastatic disease are keys to correct diagnosis
Infectious Ascites
• Exudative ascites with fluid demonstrating slightly higher attenuation (15-30 HU) than simple fluid
• Presence of peritoneal thickening/enhancement, septations, and frank loculated fluid collections (with peripheral rim enhancement) are clues to correct diagnosis
Cystic Peritoneal Metastases
• Most often result of mucinous neoplasms (ovary, GI tract)
• Nodular cystic lesions in the omentum and mesentery, but usually with associated soft tissue component, thickening/nodularity of omentum, and other evidence of widespread metastatic disease
• Large ascites common, frequently with evidence of loculation and internal complexity
• Adnexal mass of cystic density (ovarian, Krukenberg)
Physiologic Free Fluid
• Small fluid in cul-de-sac is physiologic in premenopausal females and should not be interpreted as pathologic ascites
• Free fluid always considered abnormal in a male patient
• Paracentesis with US guidance or blind tap (to discern nature of ascites) required in all patients with new onset ascites of unknown etiology or chronic ascites with fever, abdominal pain, renal insufficiency, or encephalopathy
• Sodium restriction and diuretics for transudative ascites
• Cases with refractory transudative ascites may require large volume paracentesis
Some patients may be candidates for peritoneovenous shunting (LeVeen, Denver catheters) or transjugular intrahepatic portosystemic shunt (TIPS)
• Patients with exudative ascites will not respond to salt restriction or diuretics, and only treatment is therapeutic paracentesis or treatment of underlying cause of ascites
DIAGNOSTIC CHECKLIST
Consider
• Recognize signs of exudative ascites and consider paracentesis for specific diagnosis
Image Interpretation Pearls
• High-attenuation ascites can result from vicarious excretion
(Left) Axial T2 FS MR demonstrates loculated T2 hyperintense ascites . Notice the presence of discrete nodules within the ascites fluid, reflecting the fact that this is malignant ascites in a patient with peritoneal carcinomatosis from appendiceal cancer.
(Right) Axial NECT in a patient after small bowel transplantation demonstrates fat-fluid levels within fluid collections that indicate the chylous nature of the fluid and that it represents leakage from small bowel lymphatics.
(Left) Axial CECT shows complex, loculated ascites from bile peritonitis due to a biliary injury. Lesser sac ascites, which displaces the stomach and duodenum in this case, is usually due to a local source (e.g., pancreatitis, gastric ulcer), peritonitis, or carcinomatosis.
(Right) Axial T1 FS C+ MR demonstrates loculated ascites in the pelvis. Notice the extensive peritoneal thickening and hyperenhancement more posteriorly in the pelvis, consistent with this patient’s malignant ascites and peritoneal carcinomatosis.
(Left) Axial CECT shows marked thickening of the distal stomach , compatible with malignancy. Extensive ascites is present with nodular thickening of the parietal peritoneum , indicating malignant ascites from gastric carcinoma.
(Right) Axial CECT in the same patient shows the tumor extending along the gastrocolic ligament to involve the transverse colon . Note the nodular thickening of the parietal peritoneum . GI malignancies are the most common source of malignant ascites in men.
Axial CECT shows loculated ascites due to peritoneal dialysis. Note the mass effect and contrast-enhancing wall.
Axial CECT in a cirrhotic patient shoes spontaneous bacterial peritonitis, loculation, and enhancing rim and gas .
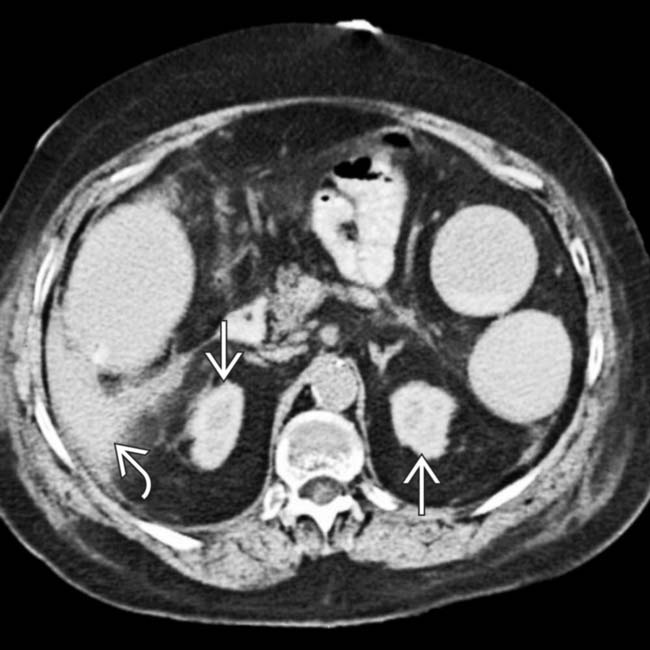
Axial NECT in a patient with pancreatitis shows a prominent lesser sac collection of fluid .
Axial CECT shows fluid in lesser sac and the “scalloped” surface of the liver and spleen. Diagnosis was peritoneal carcinomatosis.
Axial CECT shows ascites, including lesser sac, along with a thickened, “smudged” omentum . Diagnosis was malignant ascites.
Axial CECT shows loculated ascites, peritoneal thickening , and nodular omentum. Diagnosis was ovarian carcinoma metastases.
Axial CECT shows a nodular, cirrhotic liver with signs of portal hypertension, including splenomegaly, ascites , and varices . The intrahepatic ducts are dilated with an abnormal arborization due to primary sclerosing cholangitis in this case of transudative ascites.
Axial CECT shows a shattered spleen with a sentinel clot (higher density, heterogeneous) in the perisplenic region and a large hemoperitoneum. The free-flowing blood around the liver measured 35-45 HU.
Axial CECT shows long segment of jejunal thickening , mesenteric infiltration, and ascites in this patient with Henoch Schönlein purpura. Steroid treatment resulted in prompt resolution of symptoms.
Axial CECT shows fluid and nodular thickening on both sides of the diaphragm . Ascites lies medial to the diaphragm and nodular thickening on the diaphragm undersurface represents malignant implants on the parietal peritoneum . Note pleural implant .
Axial CECT in this case of TB peritonitis shows marked thickening of the omentum and peritoneum with infiltration of the mesentery, loculated ascites, and enlargement of mesenteric nodes .
Axial NECT shows dense persistent enhancement of small kidneys compatible with contrast-induced nephropathy. Ascites measured 60 HU due to vicarious excretion of the contrast medium from the peritoneum as a means of compensating for failed renal excretion.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Free-flowing ascites conforms to shape of surrounding structures and flows to dependent recesses
Simple fluid signal on T1WI (hypointense) and T2WI (hyperintense) MR
No appreciable complexity within ascites fluid
• Exudative ascites: Typically demonstrates increasing density of fluid with increasing protein content
Often mildly hyperdense (15-30 HU) relative to transudative ascites
May demonstrate complexity, including septations, peritoneal thickening/enhancement, and loculation
Loculated ascites fluid exerts mass effect and displaces adjacent structures (such as bowel loops)
Usually simple fluid signal on T1WI and T2WI MR, but internal complexity and protein can result in intermediate T1 and T2 signal
Chylous ascites can measure < 0 HU or demonstrate fat-fluid levels
PATHOLOGY
• Ascites is typically divided into 2 types
Transudative ascites is caused by high portal venous pressures and is characterized by low protein, low LDH, normal glucose, and low specific gravity
– Transudative ascites is simple ascites fluid most often caused by cirrhosis, hepatitis, heart failure, renal failure, hypoproteinemia, etc.
Exudative ascites is characterized by high protein and high specific gravity
– Exudative ascites related to multiple causes, such as infection, ischemia, peritoneal carcinomatosis, peritonitis, or pancreatitis
(Left) Axial CECT shows ascites due to hepatic cirrhosis, with large varices and splenomegaly. Notice the relatively simple, uncomplicated appearance of this transudative ascites.
(Right) Axial CECT shows massive ascites due to right heart failure. Like other forms of transudative ascites, note that the fluid appears simple without evidence of complexity, nodularity, or adjacent peritoneal thickening/enhancement.
(Left) Ultrasound shows large anechoic ascites in the lower abdomen displacing bowel loops in a patient with cirrhosis. As in this case, simple transudative ascites is classically anechoic, freely mobile, and shows acoustic enhancement.
(Right) Ultrasound shows complicated ascites in a cirrhotic patient. The fluid was non-mobile and loculated on real-time scanning, and there are multiple internal septations , suggesting this is not simple transudative ascites. The ascites fluid was found to be infected.
TERMINOLOGY
Definitions
• Pathologic accumulation of fluid within peritoneal cavity
IMAGING
General Features
• Best diagnostic clue
Diagnostic paracentesis (in cases where either infection or tumor is suspected)
• Location
Free-flowing ascites fluid flows to most dependent recesses of abdomen and pelvis
– Morison pouch (hepatorenal fossa): Most dependent recess in upper abdomen
– Rectouterine or rectovesical space: Most dependent spaces in pelvis
– Paracolic gutters and subphrenic spaces
– Lesser sac usually does not fill with ascites, with the exception of cases with tense ascites or ascites due to a local source (gastric ulcer or pancreatitis)
Otherwise, lesser sac fluid suspicious for ascites related to carcinomatosis or infection
• Morphology
Free-flowing ascites: Conforms to shape of surrounding structures and does not deform normal shape of adjacent organs or exert mass effect
– Fluid insinuates itself between organs
Loculated fluid: Fluid demonstrates rounded contour and appears encapsulated
– Loculated ascites fluid exerts mass effect and displaces adjacent structures (such as bowel loops)
• Key concepts and descriptors
Ascites typically divided into 2 types
– Transudative ascites is caused by high portal venous pressures and is characterized by low protein, low LDH, normal glucose, and low specific gravity
Transudative ascites is simple ascites fluid that is most often caused by cirrhosis, hepatitis, heart failure, renal failure, or hypoproteinemia
– Exudative ascites characterized by high protein and high specific gravity
Exudative ascites related to multiple causes, such as infection, ischemia, peritoneal carcinomatosis, peritonitis, and pancreatitis
• Abdominal radiograph: Insensitive for fluid, as diagnosis of ascites on radiographs requires a substantial amount of fluid to be present (usually > 500 cc)
Diffuse haziness and increased density of abdomen
Poor visualization of normally visualized soft tissue structures, such as psoas and renal outline
– Obliteration of hepatic and splenic angles
Bulging of flanks due to fluid distending abdomen
Separation of small bowel loops with centralization of floating gas-containing small bowel
Hellmer sign: Lateral edge of liver medially displaced from adjacent thoracoabdominal wall
Symmetric densities on sides of bladder (dog ears sign)
Medial displacement of ascending and descending colon
Lateral displacement of properitoneal fat line
CT Findings
• Transudative ascites
Typical transudative ascites has density of 0-15 Hounsfield units (HU) and appears free flowing
Small amounts of ascites typically seen in right perihepatic space, Morison pouch, and pouch of Douglas
Larger amounts of fluid accumulate in paracolic gutters
– Ascites can cause centralization of bowel loops
– Ascites accumulating in central abdomen may have triangular configuration within leaves of mesentery
Massive ascites distends peritoneal spaces
Look for associated evidence of liver, heart, or kidney failure (most common causes of transudative ascites)
• Exudative ascites
Exudative ascites typically demonstrates increasing density of fluid with increasing protein content
– Exudative ascites often mildly hyperdense relative to transudative ascites (15-30 HU)
– May demonstrate complexity, including septations, peritoneal thickening/enhancement, and loculation
Ascites related to peritoneal carcinomatosis: Complex ascites with nodularity and thickening of adjacent peritoneum and frequent loculation of ascites
Buy Membership for Radiology Category to continue reading. Learn more here









 due to hepatic cirrhosis, with large varices and splenomegaly. Notice the relatively simple, uncomplicated appearance of this transudative ascites.
due to hepatic cirrhosis, with large varices and splenomegaly. Notice the relatively simple, uncomplicated appearance of this transudative ascites.

 in the lower abdomen displacing bowel loops
in the lower abdomen displacing bowel loops  in a patient with cirrhosis. As in this case, simple transudative ascites is classically anechoic, freely mobile, and shows acoustic enhancement.
in a patient with cirrhosis. As in this case, simple transudative ascites is classically anechoic, freely mobile, and shows acoustic enhancement.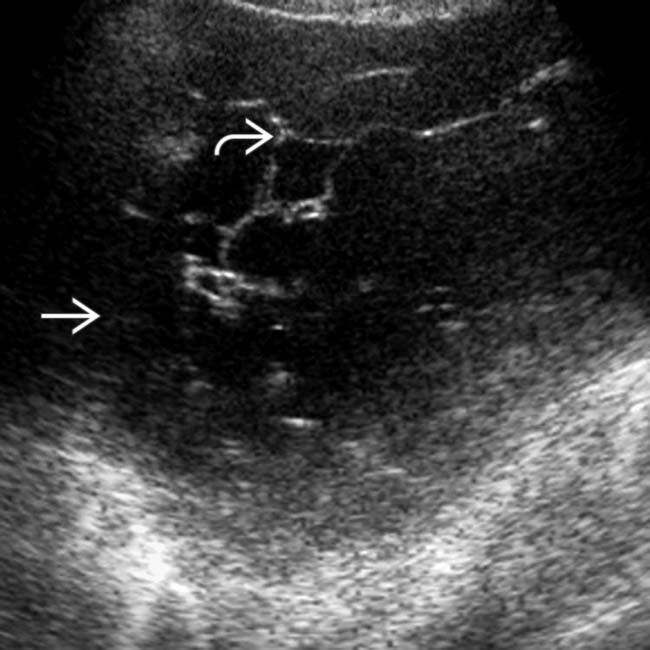
 in a cirrhotic patient. The fluid was non-mobile and loculated on real-time scanning, and there are multiple internal septations
in a cirrhotic patient. The fluid was non-mobile and loculated on real-time scanning, and there are multiple internal septations  , suggesting this is not simple transudative ascites. The ascites fluid was found to be infected.
, suggesting this is not simple transudative ascites. The ascites fluid was found to be infected.


















 Small amounts of ascites typically seen in right perihepatic space, Morison pouch, and pouch of Douglas
Small amounts of ascites typically seen in right perihepatic space, Morison pouch, and pouch of Douglas




 Exudative ascites typically demonstrates increasing density of fluid with increasing protein content
Exudative ascites typically demonstrates increasing density of fluid with increasing protein content
 Ascites related to peritoneal carcinomatosis: Complex ascites with nodularity and thickening of adjacent peritoneum and frequent loculation of ascites
Ascites related to peritoneal carcinomatosis: Complex ascites with nodularity and thickening of adjacent peritoneum and frequent loculation of ascites
 Chylous ascites: Intraperitoneal and extraperitoneal fluid usually of water density, but can be < 0 HU or demonstrate fat-fluid levels (due to fat content)
Chylous ascites: Intraperitoneal and extraperitoneal fluid usually of water density, but can be < 0 HU or demonstrate fat-fluid levels (due to fat content)
 Bile ascites: Low density fluid (usually < 15 HU) most typically localized adjacent to liver or biliary structures
Bile ascites: Low density fluid (usually < 15 HU) most typically localized adjacent to liver or biliary structures
 Urinary ascites: Low density fluid (< 15 HU) usually localized adjacent to urinary tract (and site of leak)
Urinary ascites: Low density fluid (< 15 HU) usually localized adjacent to urinary tract (and site of leak)






 Free fluid forms acute angles where fluid borders organs, should shift with changes in patient position, and should compress with increased transducer pressure
Free fluid forms acute angles where fluid borders organs, should shift with changes in patient position, and should compress with increased transducer pressure





















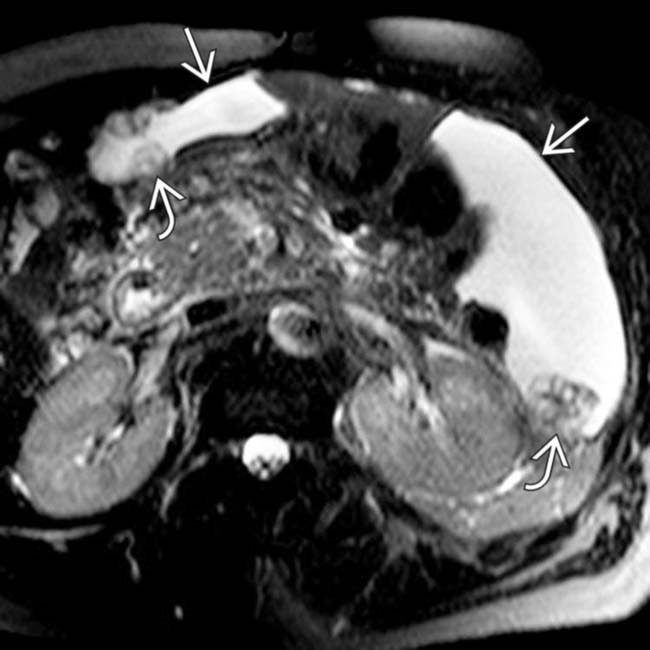
 . Notice the presence of discrete nodules
. Notice the presence of discrete nodules  within the ascites fluid, reflecting the fact that this is malignant ascites in a patient with peritoneal carcinomatosis from appendiceal cancer.
within the ascites fluid, reflecting the fact that this is malignant ascites in a patient with peritoneal carcinomatosis from appendiceal cancer.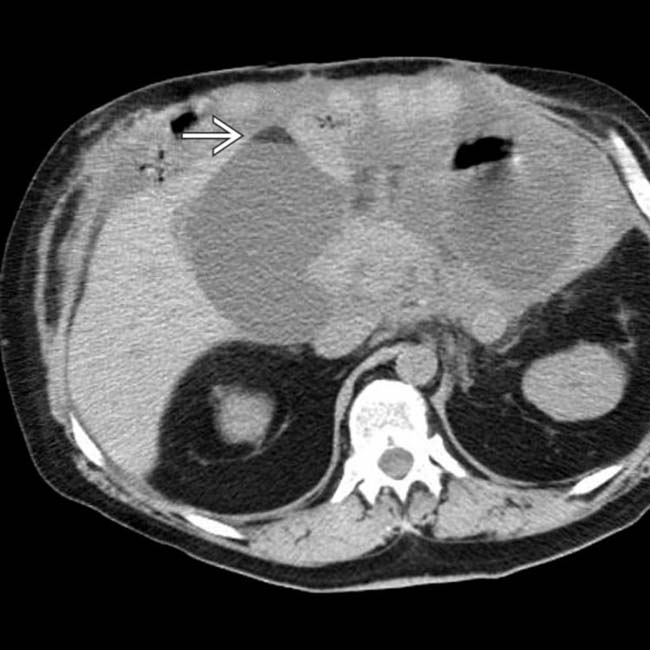
 within fluid collections that indicate the chylous nature of the fluid and that it represents leakage from small bowel lymphatics.
within fluid collections that indicate the chylous nature of the fluid and that it represents leakage from small bowel lymphatics.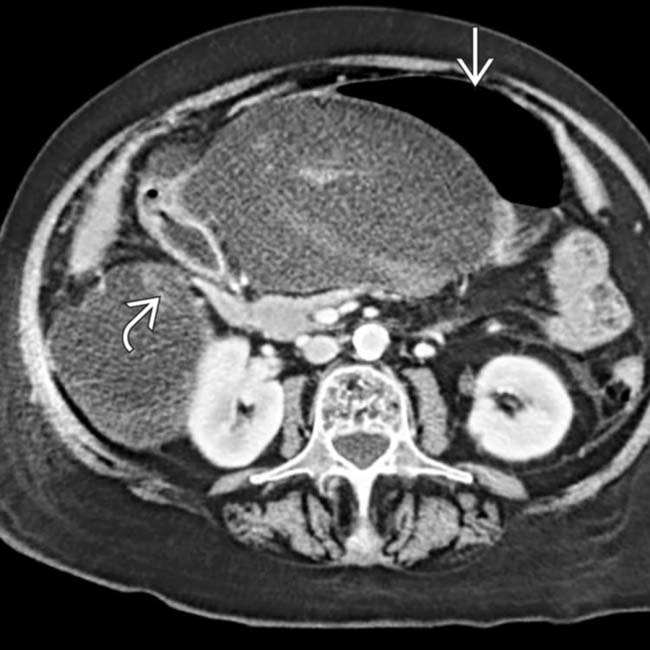
 and duodenum
and duodenum  in this case, is usually due to a local source (e.g., pancreatitis, gastric ulcer), peritonitis, or carcinomatosis.
in this case, is usually due to a local source (e.g., pancreatitis, gastric ulcer), peritonitis, or carcinomatosis.
 in the pelvis. Notice the extensive peritoneal thickening
in the pelvis. Notice the extensive peritoneal thickening  and hyperenhancement more posteriorly in the pelvis, consistent with this patient’s malignant ascites and peritoneal carcinomatosis.
and hyperenhancement more posteriorly in the pelvis, consistent with this patient’s malignant ascites and peritoneal carcinomatosis.
 , compatible with malignancy. Extensive ascites is present with nodular thickening of the parietal peritoneum
, compatible with malignancy. Extensive ascites is present with nodular thickening of the parietal peritoneum  , indicating malignant ascites from gastric carcinoma.
, indicating malignant ascites from gastric carcinoma.
 . Note the nodular thickening of the parietal peritoneum
. Note the nodular thickening of the parietal peritoneum  . GI malignancies are the most common source of malignant ascites in men.
. GI malignancies are the most common source of malignant ascites in men.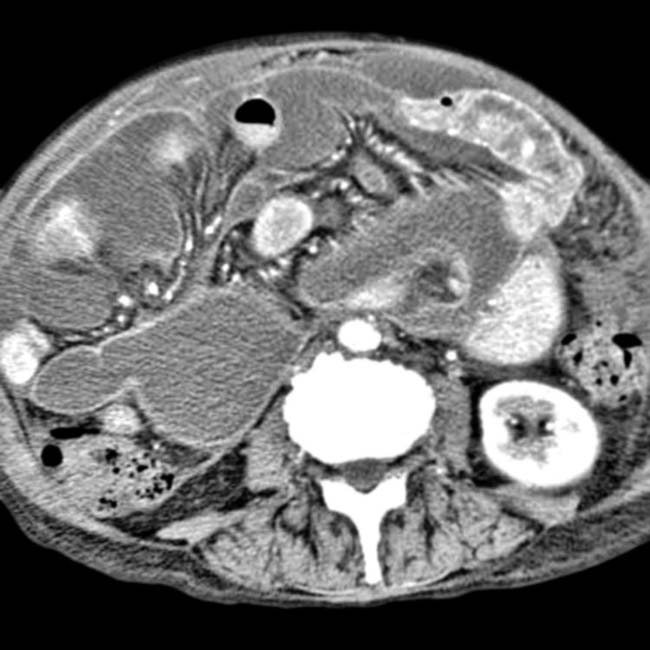

 .
.
 .
.

 . Diagnosis was malignant ascites.
. Diagnosis was malignant ascites.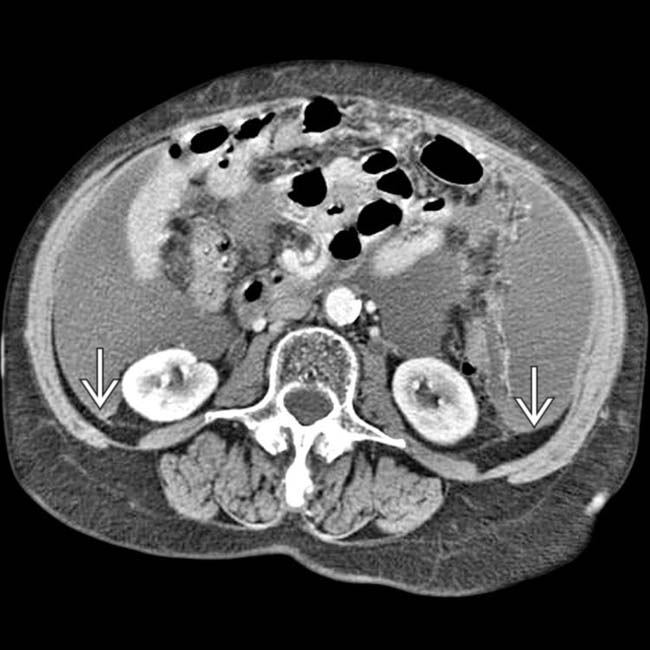
 , and nodular omentum. Diagnosis was ovarian carcinoma metastases.
, and nodular omentum. Diagnosis was ovarian carcinoma metastases.
 , and varices
, and varices  . The intrahepatic ducts are dilated with an abnormal arborization due to primary sclerosing cholangitis in this case of transudative ascites.
. The intrahepatic ducts are dilated with an abnormal arborization due to primary sclerosing cholangitis in this case of transudative ascites.
 (higher density, heterogeneous) in the perisplenic region and a large hemoperitoneum. The free-flowing blood around the liver
(higher density, heterogeneous) in the perisplenic region and a large hemoperitoneum. The free-flowing blood around the liver  measured 35-45 HU.
measured 35-45 HU.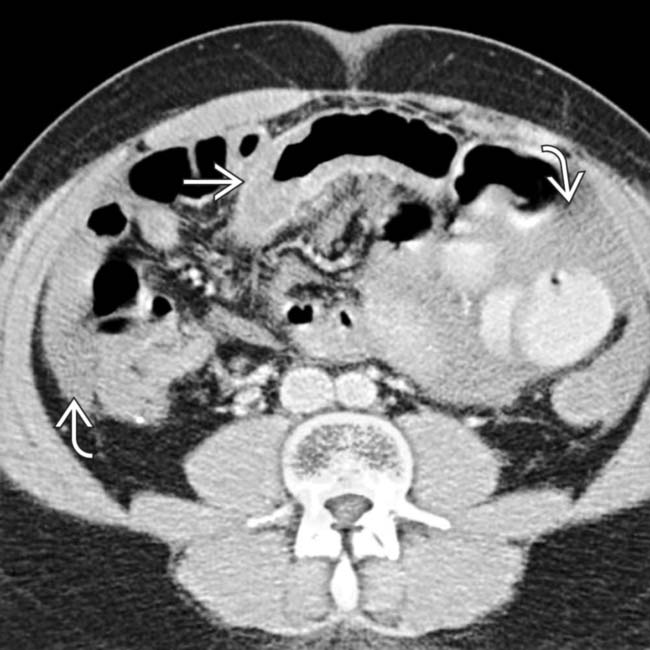
 , mesenteric infiltration, and ascites
, mesenteric infiltration, and ascites  in this patient with Henoch Schönlein purpura. Steroid treatment resulted in prompt resolution of symptoms.
in this patient with Henoch Schönlein purpura. Steroid treatment resulted in prompt resolution of symptoms.
 . Ascites lies medial to the diaphragm and nodular thickening on the diaphragm undersurface represents malignant implants on the parietal peritoneum
. Ascites lies medial to the diaphragm and nodular thickening on the diaphragm undersurface represents malignant implants on the parietal peritoneum  . Note pleural implant
. Note pleural implant  .
.
 with infiltration of the mesentery, loculated ascites, and enlargement of mesenteric nodes
with infiltration of the mesentery, loculated ascites, and enlargement of mesenteric nodes  .
.
 compatible with contrast-induced nephropathy. Ascites
compatible with contrast-induced nephropathy. Ascites  measured 60 HU due to vicarious excretion of the contrast medium from the peritoneum as a means of compensating for failed renal excretion.
measured 60 HU due to vicarious excretion of the contrast medium from the peritoneum as a means of compensating for failed renal excretion.