[level-membership-for-orthopaedics-category]
CHAPTER 16 Arthroscopic Triceps Repair
PATIENT EVALUATION
History and Physical Examination
The physical examination begins with observation for swelling or ecchymosis (Fig. 16-1). Patients with complete tears may have a complete loss of the ability to extend the elbow, whereas those with partial or degenerative tears may retain active extension but in a weakened state. In those with the more subtle tears, trying to extend the elbow from a fully flexed position reproduces pain directly over the site of the injury (i.e., triceps stress test), which can then be palpated for a defect.

TREATMENT
Arthroscopic Technique
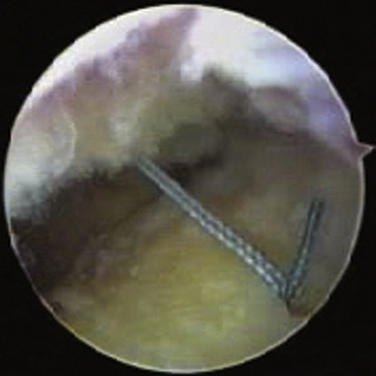
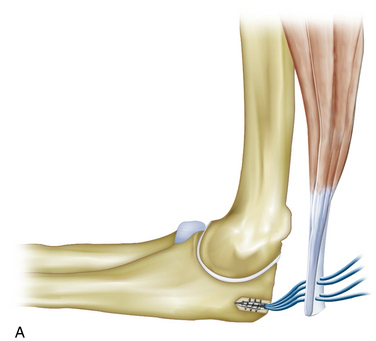
The initial portal into the posterior aspect of the elbow is the posterior central portal, located approximately 3 cm above the tip of the olecranon. In most triceps avulsions, this portal goes through the tear. A posterior lateral portal is then established, and the injury to the tendon is visualized (Fig. 16-2). The arthroscope is moved to the posterior lateral portal, and the shaver is introduced through the posterior central portal. The ulnar insertion is identified and lightly débrided, as are the edges of the torn tendon. A central olecranon bursa portal is then established, and a dual-sutured anchor is inserted at the proximal olecranon tip, angling toward the coronoid base to prevent inadvertent penetration through the articular surface (Fig. 16-3).
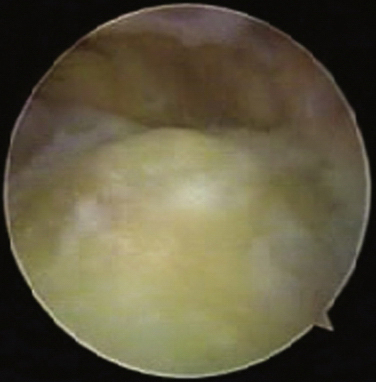
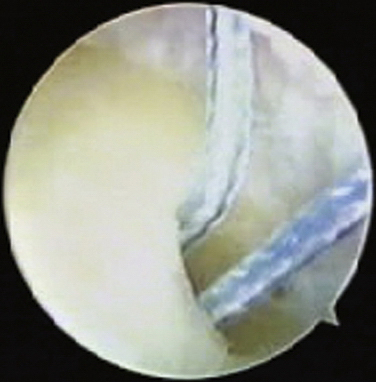
FIGURE 16-3 The first anchor is placed into the proximal part of the olecranon in preparation for repair.
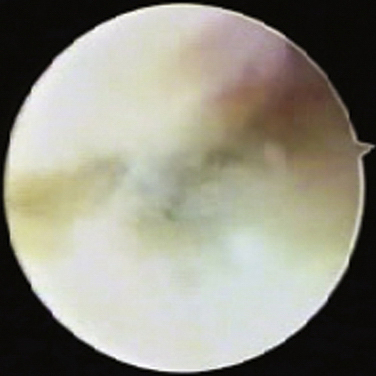
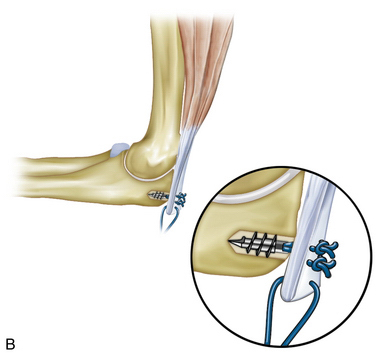
A retrograde retriever is then placed percutaneously through the medial and lateral aspects of the muscle-tendon junction of the triceps and is used to retrieve a suture through this area of the tendon (Fig. 16-4). Two mattress stitches are usually required to complete the proximal part of the repair (Fig. 16-5). The first set of sutures is retrieved percutaneously, and a sliding knot is tied to lock down the proximal attachment of the triceps and seal the joint. The second set of sutures is retrieved through the tendon and tied. The arthroscope is then placed into the olecranon bursa, and a second anchor is placed more distally in the ulna. These sutures are retrieved through the end of the tendon in a simple fashion to complete the repair (Fig. 16-6).
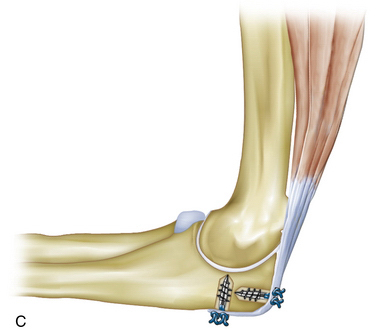
In an alternative technique, both anchors are placed before any suture shuttle or retrieval is undertaken. The proximal and distal sutures are then retrieved and tied. The sutures may be crossed to create a suture bridge that holds the tendon down to the bone.
1. Morrey B. Rupture of the triceps tendon. In: Morrey B, editor. The Elbow and its Disorders: Expert Consult. 4th ed. Philadelphia, PA: WB Saunders; 2009:536-546.
2. Armando F, Vidal AF, Drakos MC, Allen AA. Biceps tendon and triceps tendon injuries. Clin Sports Med. 2004;23:707-722.
3. Daglar B, Delialioglu OM, Ceyhan E, et al. Combined surgical treatment for missed rupture of triceps tendon associated with avulsion of the ulnar collateral ligament and flexor-pronator muscle mass. Strat Traum Limb Recon. 2009;4:35-39.
4. Rineer CA, Ruch DS. Elbow tendinopathy and tendon ruptures: epicondylitis, biceps and triceps ruptures. J Hand Surg Am. 2009;34:566-576.
5. Belentani C, Pastore D, Wangwinyuvirat M, et al. Triceps brachii tendon: anatomic-MR imaging study in cadavers with histologic correlation. Skeletal Radiol. 2009;38:171-175.
6. Morrey B. Rupture of the triceps tendon. In: Morrey B, editor. The Elbow and its Disorders. 3rd ed. Philadelphia, PA: WB Saunders; 2000:479-484.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
CHAPTER 16 Arthroscopic Triceps Repair
PATIENT EVALUATION
History and Physical Examination
The physical examination begins with observation for swelling or ecchymosis (Fig. 16-1). Patients with complete tears may have a complete loss of the ability to extend the elbow, whereas those with partial or degenerative tears may retain active extension but in a weakened state. In those with the more subtle tears, trying to extend the elbow from a fully flexed position reproduces pain directly over the site of the injury (i.e., triceps stress test), which can then be palpated for a defect.
