8. Arthrogryposis
Definition
Arthrogryposis is a nonprogressive condition that is obvious at birth by the characteristic multiple joint contractures that occur throughout the body. The disorder is also known as arthrogryposis multiplex congenita.
Incidence
The incidence of arthrogryposis is about 1:3000 live births without racial or gender preference.
Causes of Fetal Akinesia
• Attempted pregnancy termination
• Carbon monoxide poisoning or severe hypoxia during pregnancy
• Chronic amniotic fluid leak
• Demise of a twin
• Infants of mothers with myotonic dystrophy, myasthenia gravis, multiple sclerosis
• Large uterine fibroids or tumors
• Maternal fever >39° C (>102.2° F) for an extended time
• Maternal hyperthermia
• Maternal infections (rubella, rubeola, coxsackievirus, enterovirus, or Akabane)
• Multiple fetuses
• Oligohydramnios
• Severe hypotension at a critical time
• Teratogens (drugs, alcohol, curare, methocarbamol, phenytoin)
Etiology
The underlying cause of arthrogryposis is fetal akinesia. Fetal abnormalities—such as neurogenia, muscular or connective tissue disorders, limitations to mechanical movement—or maternal disorders—such as infections, substance abuse, trauma, or maternal illness—may be the cause of fetal akinesia. Fetal akinesia results in development of excess connective tissue around the joint. The joint becomes fixed and the limited movement within the uterus further exacerbates the joint contracture.
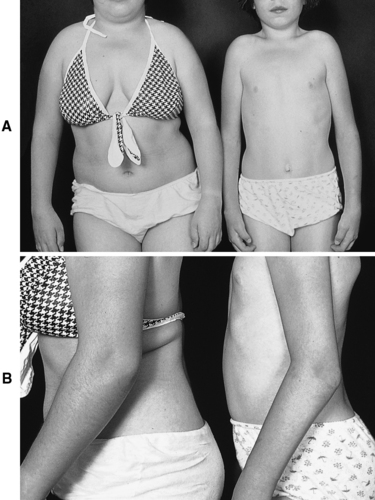 |
| Arthrogryposis. A, Two sisters with the generalized form of the disorder. Note the stiff posture and tubular appearance of the limbs. Motion of all joints is limited as a result of failure in the development of or degeneration of muscular structures. Their stature is short. B, The lateral view highlights the flexion of contractures of the elbows. |
Syndromes Associated with Arthrogryposis
• Bowen-Conradi syndrome∗
• C syndrome (Opitz trigonocephaly syndrome) ∗
• Faciocardiomelic syndrome∗
• Fetal alcohol syndrome
• FG syndrome∗
• Marden-Walker syndrome∗
• Meckel syndrome∗
• Mietens syndrome∗
• Miller-Dieker syndrome
• Syndrome of cloudy cornea/diaphragmatic defect/distal limb deformities
• Toriello-Bauserman syndrome∗
• Zellweger syndrome∗
∗See Appendix G: Rare Syndromes.
Signs and Symptoms
• Absence of muscles or muscle groups
• Absent patella
• Aortic stenosis
• Cleft palate
• Coarctation of the aorta
• Craniosynostosis
• Cryptorchidism
• Cutis marmorata
• Cyanotic heart disease
• Dislocated radial heads
• Distally increasing severity of deformity
• Facial asymmetry
• Flat nasal bridge
• Fusiform or cylindrical shape of involved extremities
• Hemangioma
• Hypertelorism
• Hypoplastic diaphragm
• Inguinal/umbilical hernia
• Joint dislocations
• Joint rigidity
• Lack of labia
• Limb shortening
• Limited jaw range of motion
• Microencephaly
• Micrognathism
• Microphallus
• Muscle atrophy
• Pterygia across joints
• Ptosis
• Pulmonary hypoplasia
• Renal anomalies
• Scoliosis
• Strabismus
• Symmetric deformities
• Tracheal and/or laryngeal clefts or stenosis
• Trismus
Medical Management
Medical management of arthrogryposis consists primarily of physical therapy. The goal is to attain and maintain limb alignment and establish joint stability so the patient will eventually be able to ambulate. Gentle manipulation and stretching result in improved range of motion. Best results are obtained when therapy is initiated soon after birth. Late manipulation is not very productive. Casting for immobility is somewhat counterproductive. Splinting overnight is preferred in combination with physical therapy.
The patient who has severe trismus may require feeding assistance, such as a feeding gastrostomy or nasogastric feeding tube. The patient may require intubation or tracheostomy for respiratory support.
Surgical intervention is sometimes required. At an early age, such as 3 to 12 months, a single-stage bone and tendon transfer procedure should be undertaken. More intricate procedures, such as opponensplasty, may be contemplated at later developmental/growth stages to improve function. Generally, soft tissue procedures are performed at an early age; osteotomies are performed only after growth is completed. Specific joints are generally addressed individually.
Complications
• Craniofacial deformities
• Fractures
• Osseous hypoplasia
• Scoliosis
Anesthesia Implications
The patient who requires feeding assistance may be chronically dehydrated and may have electrolyte imbalances. Similar to a patient with muscular diseases, the patient with arthrogryposis may experience heightened sensitivity or other altered responses to muscle relaxants, both depolarizing and nondepolarizing.
Of particular importance is the association of malignant hyperthermia in the patient who has a form of arthrogryposis with multiple pterygium syndrome.
Vascular access may be difficult to obtain in part because of the joint contractures.
Thorough cardiac assessment should be completed preoperatively. The patient with arthrogryposis is prone to cardiac anomalies, including aortic stenosis, coarctation of the aorta, and cyanotic heart disease.
The patient with arthrogryposis may have craniofacial anomalies such as micrognathia or high-arched palate as well as cervical spine abnormalities. As a result, securing the patient’s airway may prove difficult and may be deemed impossible. The fiberoptic bronchoscope, intubating laryngeal mask airway, and other difficult airway equipment should be immediately on hand. If these measures prove unsuccessful, a tracheostomy may be required. In addition, the patient’s normal respiratory function may be a very precarious balance because of associated malformations such as tracheal and laryngeal clefts, and/or stenosis, weak muscles, hypoplasia, or hypoplastic diaphragm. Therefore the anesthetist should anticipate the need for postoperative ventilatory support.
The multiple joint contractures may make it difficult to position the patient. Positioning must also be undertaken with care and caution to minimize the risk of fractures.






