12 Approach and Techniques
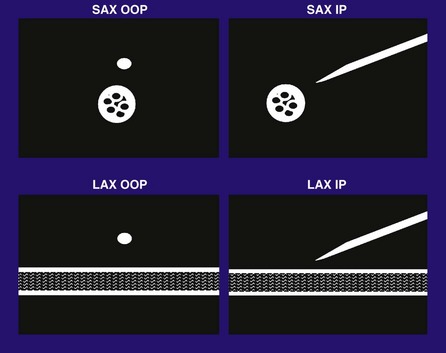
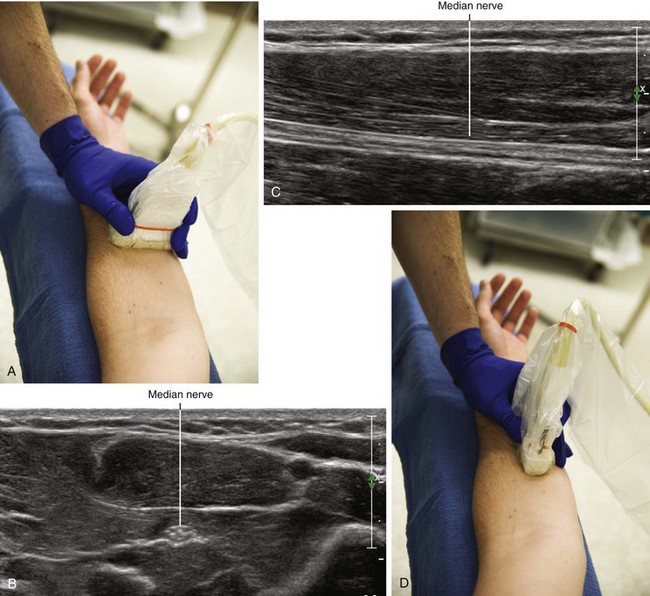
Out-of-Plane Approach
There are several advantages to the out-of-plane approach to regional block (Table 12-1). This approach is most similar to traditional approaches to regional block guided by nerve stimulation or palpation. Therefore, the out-of-plane approach provides a natural transition from one form of guidance to another. The out-of-plane approach uses a shorter needle path than in-plane approaches. If short-axis views of the nerve are used, an out-of-plane approach results in catheter placement that is guided along the path of the nerve. One disadvantage of the out-of-plane approach is the extent of the unimaged needle path (structures that may lie short of or beyond the scan plane). If the needle tip crosses the scan plane without recognition, it can be advanced beyond the scan plane into undesired tissue.
Table 12-1 Comparison of Out-of-Plane and In-Plane Approaches
| Approach | Advantages | Disadvantages |
|---|---|---|
| Out-of-plane (OOP) | Most similar to other approaches to regional block (nerve stimulation or palpation) Shorter needle path than with in-plane approaches Along the nerve path (catheters) |
Unimaged needle path, crossing the plane of imaging without recognition |
| In-plane (IP) | Most direct visualization | Partial line-ups (creating a false sense of security when the needle tip is not correctly identified) Some unimaged needle path occurs with IP approach, but typically less than with OOP approach Longer paths and therefore more structures to cross with the block needle |
In-Plane Approach
External marks on the transducer can be used to guide needle placement for in-plane technique. However, the mechanical axis of the transducer and its acoustic axis are not always precisely aligned.1
Offline Markings
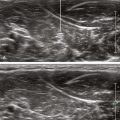
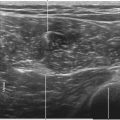
Offline techniques involve external skin markings from ultrasound scans without imaging during needle placement. Changes in patient position, mobility of the skin, and dynamic changes with needle placement and injection limit the utility of this approach. The skin adjacent to the sides of the transducer can be marked. Alternatively, a paper clip or solid metal stylet (preferably with dull ends) can be used to create artifact within the field to mark the position of the object. For this technique, spatial compound imaging should be turned off to enhance the artifact.2 The M-mode center line can be used to facilitate offline markings in the center of the field.
1 Goldstein A, Parks JA, Osborne B. Visualization of B-scan transducer transverse cross-sectional beam patterns. J Ultrasound Med. 1982;1:23–35.
2 Gabriel H, Shulman L, Marko J, et al. Compound versus fundamental imaging in the detection of subdermal contraceptive implants. J Ultrasound Med. 2007;26:355–359.