Appendectomy
In the past, removal of the appendix was electively performed by gynecologists during laparotomy. Now, this practice is less commonly carried out for a variety of reasons, including medical liability risks, perceived advantage for retention of the appendix, lack of informed consent, and lack of technical know-how. Clearly, the latter two concerns can be remedied by explaining the advantages and disadvantages of the procedure to the patient preoperatively and obtaining permission for including the procedure during the proposed laparotomy. Lack of technical know-how requires that the gynecologist or resident be supervised and taught the technique of appendectomy. Obviously, the best scenario for teaching the appendectomy operation is during elective surgery. Patients who have undergone salpingostomy for tubal pregnancy, tubal reconstruction, or treatment for pelvic inflammatory disease and those who have severe adhesions are candidates for routine appendectomy. Similarly, fecoliths identified by computed axial tomography (CAT) scan or by palpation are reasonable indications for incidental appendectomy.
The cecum and ileocolic junction are identified. The cecum is elevated, and the appendix, together with its blood supply (in the mesoappendix), is noted. The terminal portion of the appendix is grasped with a Babcock clamp and placed on stretch. A window through the mesoappendix is tunneled between the cecum and the appendiceal artery. Usually an avascular clearing in the mesentery can be seen. Kelly clamps are placed in pairs along the axis of the appendix across the mesoappendix. The mesentery is progressively cut between the clamps until the base of the appendix and the cecum are reached (Fig. 97–1). Next, a purse string stitch of 2-0 silk or 3-0 Vicryl is stitched into the muscularis of the cecum surrounding the base of the appendix. Two Kelly clamps are placed across the proximal portion of the now freed appendix. The first clamp is juxtaposed to the cecum. A third Kelly clamp crushes the appendix between the point where the first and second clamps have been secured. A ligature is then applied across the appendix in the crush zone. The appendix is incised between the first and second clamps but above the ligature (Fig. 97–2A); it is placed in a formalin-containing specimen jar. A second ligature of 3-0 Vicryl is tied beneath clamp #1 (Fig. 97–2B). The doubly tied appendiceal stump is inverted into the center of the cecal purse string suture (Fig. 97–2C). The purse string is tightened, thereby burying the appendiceal stump. The purse string is tied (Fig. 97–2D). The surgical site is irrigated with normal saline and checked for bleeding. Alternatively, during laparoscopy or laparotomy, the appendix can be rapidly removed by using the surgical stapler (Fig. 97–3).
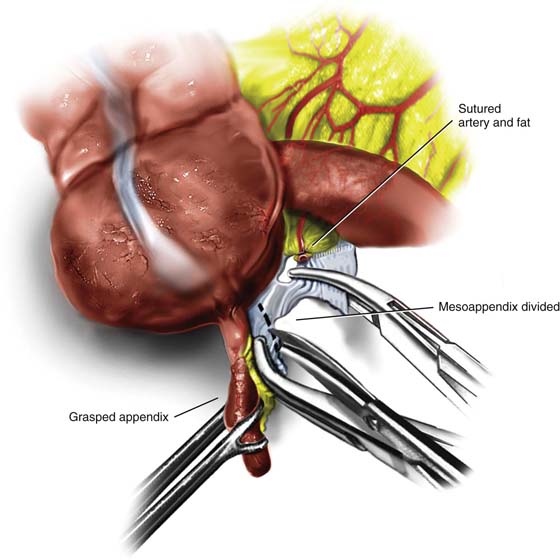
FIGURE 97–1 The distal portion of the appendix is secured with a Babcock clamp. A window has been developed in the mesoappendix, and a Kelly clamp has been placed along the mesentery to secure the blood supply. A 3-0 Vicryl suture ligature has been placed and tied. The Kelly clamp has been moved forward. Kelly clamps have been placed along the mesentery close to the appendix. The mesentery is cut between the clamps.
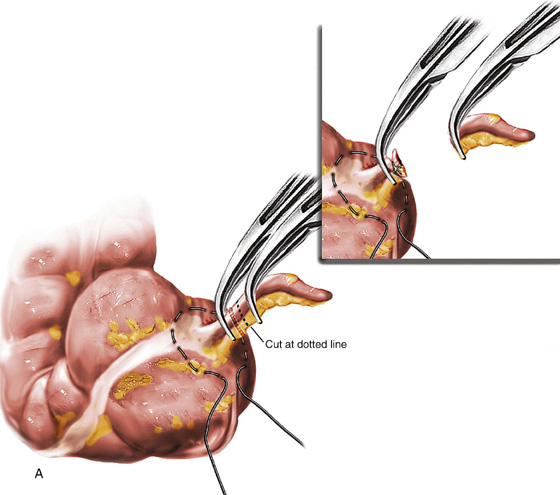
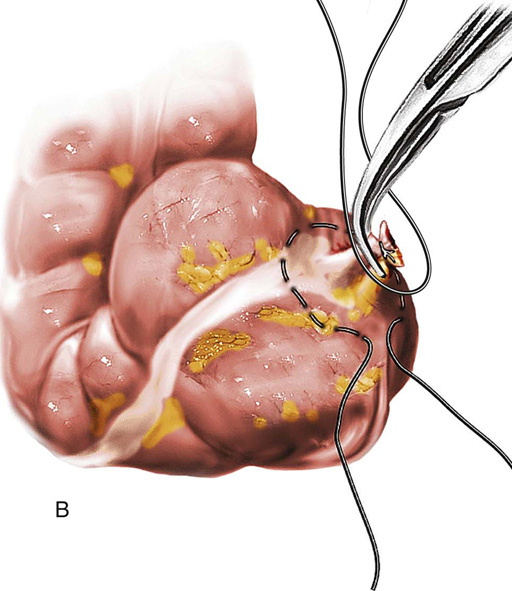

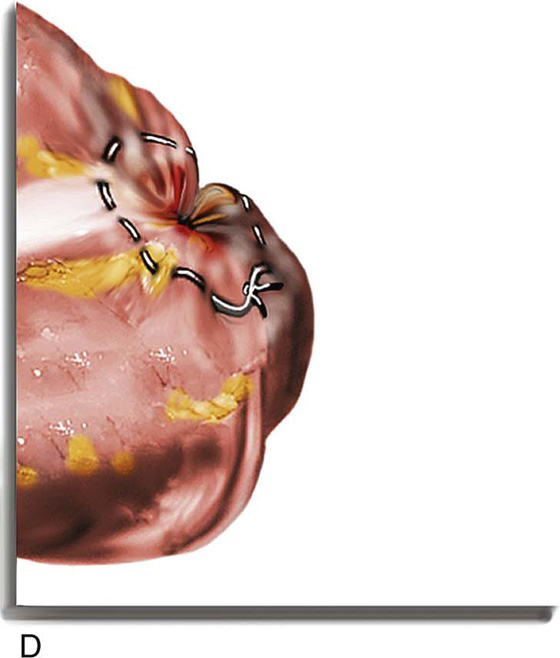
FIGURE 97–2 A. Two (1 and 2) Kelly clamps have been placed across the proximal appendix. A third clamp has been removed and a 3-0 Vicryl ligature tied in the crushed area. Alternatively, the appendix could be cut between the clamps, and a single ligature could be tied beneath clamp #1. Inset. The appendix has been cut between the first ligature and the second applied clamp (clamp #2). B. A purse string suture of 2-0 silk is placed into the cecum at the base of the appendix. C. A 3-0 Vicryl ligature is tied beneath clamp #1. The appendiceal stump is now doubly ligated. Some surgeons prefer at this point to apply phenol to the end of the stump by using a cotton-tipped applicator. D. The stump is inverted into the purse string. The latter is tightened and tied.
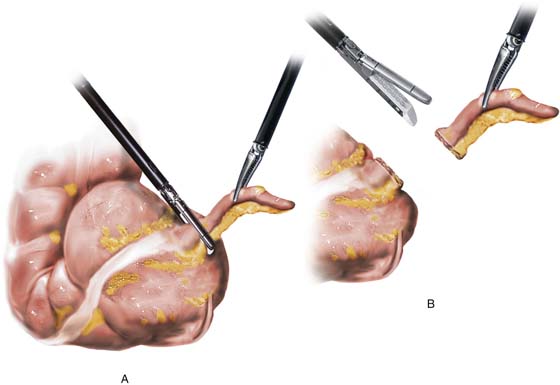
FIGURE 97–3 A. A laparoscopic curved clamp grasps the appendix. B. A laparoscope stapling device seals and cuts the appendix at the base.






