44 Anterior Sciatic Nerve Block
Suggested Technique
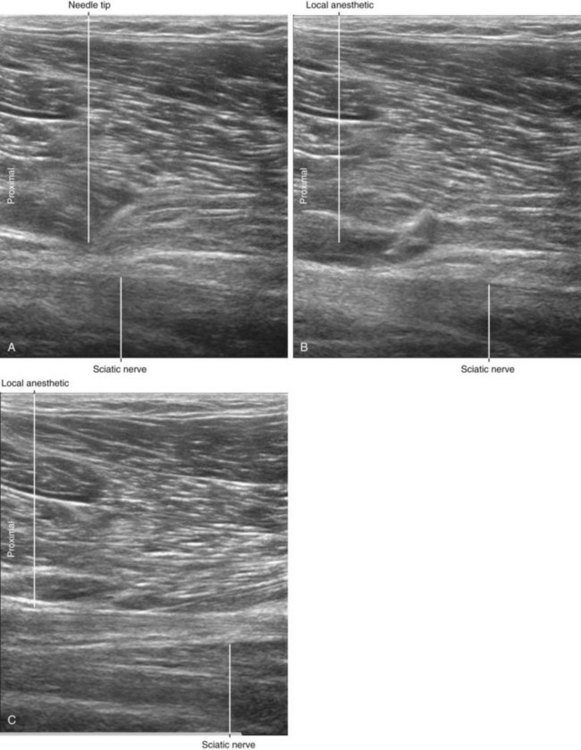
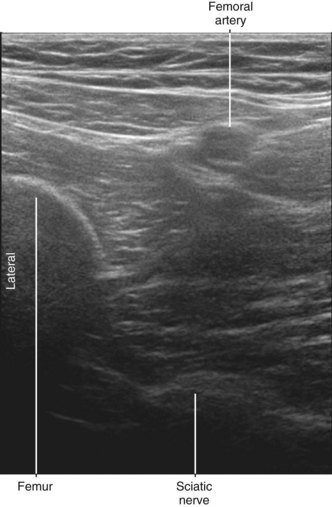
In many patients the sciatic nerve is easy to identify because it appears as a hyperechoic, linear (cable-like) structure deep to the clearly delineated border of the adductor magnus muscle that is formed by the intermuscular septum.1 Because this block is performed distal to the lesser trochanter of the femur, external rotation of the leg promotes access to the sciatic nerve.2
Clinical Pearls
• The sciatic nerve is approximately 6 to 10 cm from the anterior surface of the thigh. Although the nerve is deep its visibility is enhanced in long-axis view deep to the distinct border of the adductor magnus muscle.
• The anterior approach to sciatic nerve block is usually performed 2 to 5 cm distal to the lesser trochanter of the femur. The lesser trochanter is the bony prominence on the anteromedial aspect of the femur to which the iliopsoas tendon attaches.

1 Tsui BC, Ozelsel TJ. Ultrasound-guided anterior sciatic nerve block using a longitudinal approach: “expanding the view.”. Reg Anesth Pain Med. 2008;33(3):275–276.
2 Vloka JD, Hadzić A, April E, et al. Anterior approach to the sciatic nerve block: the effects of leg rotation. Anesth Analg. 2001;92(2):460–462.