Answers
Case 1
In a patient such as this, with moderate hypoxaemia and no ventilatory impairment, monitoring by pulse oximetry is more appropriate than repeated ABG sampling. Indications for further ABG analysis would include signs of exhaustion or hypercapnia (p. 23) or a further significant decline in SaO2.
Case 2
The likeliest cause of chronic type 2 respiratory impairment in this case is severe obesity. Around 20% of individuals with a body mass index greater than 40 have chronic hypercapnia from restricted ventilation (pickwickian syndrome).
Case 4
In addition to basic life support measures, he should be administered an opioid antagonist (e.g. naloxone), to reverse the respiratory depression, then closely monitored to ensure sustained improvement.
Case 5
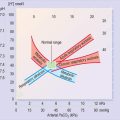
Although this patient is likely to have a chronically low PaO2, the acute deterioration in his symptoms and exercise tolerance suggests a further recent decline from his normal baseline. Importantly, even a small drop in PaO2 around this level (steep part of O2–Hb curve) may cause a marked reduction in SaO2, compromising O2 delivery to tissues. Thus O2 is required both to alleviate symptoms and to prevent the development of tissue hypoxia, and should not be withheld for fear of precipitating hypoventilation.
Case 6
Remember that, with acute respiratory acidosis, there is no time for metabolic compensation to develop and a dangerous acidaemia develops rapidly. Adequate ventilation must be restored, as a matter of urgency, to correct the PaCO2. Possible measures, in this case, include a respiratory stimulant (e.g. doxapram) or, preferably, non-invasive ventilation. If these fail, intubation and mechanical ventilation may be required, if considered appropriate.
Case 7
b) Mild respiratory alkalosis balanced by mild metabolic acidosis (likely two primary processes)
The history, examination findings and chest X-ray all suggest a diagnosis of aspiration pneumonia.
This patient is severely unwell and any further decline in her PaO2 could be catastrophic (on the steep part of the O2–Hb saturation curve). Her O2 therapy should be adjusted as necessary to maintain her SaO2 above 92% and she should be managed on a high-dependency unit with close monitoring for signs of deterioration.
Case 8
Case 9
The latter point is well illustrated in this case as the patient now has life-threatening acute-on-chronic respiratory failure despite a normal SaO2. The rising PaCO2 must be rapidly checked and reversed through improving ventilation. Potential strategies include reducing inspired O2 concentration, respiratory stimulants or assisted ventilation.
Case 10
The intensive care unit should be informed immediately of any patient with acute severe asthma and life-threatening features. Patients must receive intensive treatment and monitoring, including repeated ABG measurements to assess response and identify the need for intubation.
Case 11
Care must be taken in ruling out other cardiovascular and respiratory pathologies before ascribing symptoms of chest pain and shortness of breath to psychogenic hyperventilation.
Case 12
Why does SaO2 appear to be normal?
Most pulse oximeters are unable to distinguish carboxyhaemoglobin from oxyhaemoglobin, so fail to reflect the true SaO2 in CO poisoning. In ABG analysis, the SaO2 is not normally measured but simply calculated from the measured PaO2. The latter parameter is based only on free, unbound O2 molecules so is unaffected by the presence of CO.
Case 13
For the same reason supplemetal O2 would also fail to improve O2 content significantly. Indeed the only effective strategy is to increase Hb concentration. This could be achieved rapidly, by a blood transfusion or more gradually by iron replacement.
Case 14
Mesenteric ischaemia is a difficult diagnosis to make, as presenting symptoms, signs and routine investigations are all non-specific. The diagnosis should be considered in patients with minimal abdominal examination findings despite severe pain, especially in the presence of a lactic acidosis.
Case 15
An equally important problem in diabetic ketoacidosis is the profound osmotic diuresis resulting from hyperglycaemia that leads to severe dehydration and electrolyte loss.
Case 16
Anion gap = (Na {136} + K {4.5}) – (Cl {99} + HCO3 {9.5}) = 140.5 – 108.5 = 32
Treatment for methanol poisoning is complex but often involves the administration of ethanol, which inhibits the conversion of methanol to its more toxic metabolites.
Case 18
b) Compensated metabolic acidosis or metabolic acidosis with concomitant respiratory alkalosis
The diagnosis would be confirmed in this instance by taking salicylate levels.
Case 19
In addition to basic life support and fluid resuscitation, the main intervention likely to improve this patient’s condition is the administration of intravenous hydrocortisone.
Case 20
| 1. | a) Normal (i.e. satisfactory ventilation and oxygenation being achieved by bag and mask) | |
| b) Severe metabolic acidosis (uncompensated) | ||
| 2. | Prognosis | Very poor |
This patient has a grave prognosis. The level of acidosis is unlikely to be compatible with life and, given his unfavourable rhythm (an agonal rhythm does not respond to DC cardioversion and often signifies a ‘dying heart’), age and co-morbidities, successful resuscitation is extremely unlikely.
Case 21
The patient should be transferred immediately to a critical care environment for intensive monitoring and supportive treatment.
Case 22
| 1. | a) Mild type 2 respiratory impairment (compensatory response) | |
| b) Compensated metabolic alkalosis | ||
| 2. | Electrolytes | Hypokalaemia (↓K) |
| Hyponatraemia (↓Na) | ||
| Hypochloraemia (↓Cl) | ||
| 3. | Treatment | Fluid and electrolyte replacement |
Thus, in this case, intravenous replacement of fluid and electrolytes (Na, Cl, K) would allow the kidneys to excrete more HCO3, correcting the alkalosis.
Case 23
Secondly, there is minimal respiratory compensation. Given the severe alkalaemia, one would predict a greater rise in PaCO2. This is probably explained by the child’s distress, which provides an additional respiratory stimulus blunting the compensatory response (i.e. a mild primary respiratory alkalosis).
Case 24
| 1. | a) Appearance of severe type 1 respiratory impairment | |
| b) Normal acid-base status | ||
| 2. | Explanation | Venous sample |
It is important to ensure that an ABG sample is obtained from an artery before using it to assess the PaO2. In addition to the points above, non-pulsatile flow and the need to draw back on the syringe at the time of sampling suggest venous blood.