Pruritus Ani
Pruritus ani is itching around the anal canal. It is a common symptom and in approximately half of the cases, no cause can be found.
Causes
History
Anal discharge
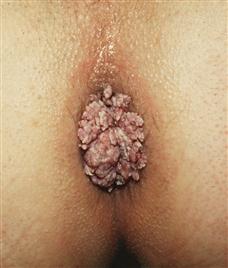
Any cause within the anus or lower rectum that produces moisture and sogginess of the anal skin may cause pruritus ani. Patients may volunteer the information that they have haemorrhoids or perianal warts. They may have noticed an anal discharge, which soils the underwear. Check for a history of anal sexual exposure.
Faecal soiling
The patient may complain of incontinence. This may be associated with poor hygiene. Chronic diarrhoea may be responsible. There may be an underlying cause for the chronic diarrhoea, e.g. colitis or Crohn’s disease. Excessive sweating in hot weather may be associated with pruritus ani.
Skin diseases
If the patient is diabetic or immunosuppressed, candidiasis may be responsible. Recent oral antibiotic therapy may result in candidiasis. Check whether the patient has an itchy rash anywhere else. This may be particularly so with scabies or eczema. Contact dermatitis may result from the use of deodorants or a change in washing powder for the underwear. Psoriasis is not usually itchy but sometimes considerable itching occurs, especially if the area becomes infected. Lichen sclerosus is uncommon, occurring chiefly in women, when it may involve both the vulva and the perineum. In men, this may be associated with balanitis xerotica obliterans, so enquire if there is any abnormality of the foreskin.
Psychogenic
Idiopathic pruritus may occur in people with anxiety states. An itch-scratch cycle may occur, which is difficult to break.
Examination
Anal discharge
Inspection of the anus may show skin tags, the external opening of a fistula-in-ano, perianal warts or haemorrhoids. Digital rectal examination may reveal a carcinoma of the anal canal or fibrous anal polyps. Proctoscopy and sigmoidoscopy will confirm any associated anal or rectal lesion. Take a swab if purulent discharge.
Faecal soiling
Soiling of the underwear may be apparent. General poor hygiene may also be apparent in the patient. Carry out a digital rectal examination to check for sphincteric tone.
Skin diseases
Candidiasis may occur in those on long-term antibiotics, diabetics and the immunosuppressed. Tinea cruris is more common in men. The infection often involves the groin and perineum in addition to the perianal areas. The patient may also have co-existing tinea pedis. With lichen sclerosus, there are well-defined plaques of superficial atrophy of the epidermis with a whitish colour. In the male, check the penis for balanitis xerotica obliterans. With contact dermatitis, there may be changes in the skin in other areas apart from the perianal area. With scabies, there are usually lesions on other parts of the body. Burrows 5–10 mm deep appear as long ridges, which may be ‘S’-shaped. Isolation of the organism with a pin and examination under the microscope will confirm the diagnosis. With psoriasis there will usually be lesions on other areas of the body, and this will also be so with eczema.
Parasites
Threadworms may be visible around the anus.
Psychogenic
There may be an obvious history of psychiatric illness or the patient may appear anxious or depressed.
General Investigations
■ FBC, ESR
These are usually normal.
■ Urinalysis
Positive for sugar – diabetic.
■ Stool culture
Ova, parasites and cysts, cause of diarrhoea.
■ Anal swab
Gram stain – Gram-negative intracellular diplococci in gonorrhoea.
■ Skin scrapings
For mycotic infection, microscopy and culture.



