Chapter 1 An introduction to cardiorespiratory physiotherapy
respiratory assessment
1.1 The scope of respiratory physiotherapy
Patients with respiratory problems are encountered in many different settings, from long-term care in the community to critically ill patients on an intensive therapy unit (ITU) (also known as critical care) (Figs 1.1–1.3). Respiratory care may be an integral part of the patient’s management in secondary care (hospital) settings, such as respiratory, medical, and surgical and orthopaedic wards as well as burns, care of the elderly, paediatric, neurological, neurosurgical and oncology units. It may also be required for patients with mental health problems or learning disabilities. Physiotherapists work in many of these settings and also within primary care (in the community) for the longer-term rehabilitation of these patients. They may be employed in multiprofessional ‘rapid response’ or ‘early discharge’ teams, in which they share the responsibility for assessing and managing acutely ill patients in their own home.



The case history in Box 1.1 illustrates the scope of respiratory physiotherapy.
1.2 Why do we assess?
When assessing a patient you should have a clear idea of the purpose of the assessment before you start. There may be several aims of a ‘respiratory’ assessment (see 1.3 Aims of respiratory assessment); although all or most of these issues may need to be addressed at some point, it is necessary to prioritize which are the most significant at the time of assessment. Be aware that priorities may change, and you need to be flexible and responsive to changes in the patient’s condition and situation.
1.3 Aims of respiratory assessment
Assessment may be carried out in order to:
• identify patients requiring immediate CPR (cardiopulmonary resuscitation) – patient safety!
• identify the need for respiratory support – such as oxygen therapy or ventilation
• identify patients requiring specific physiotherapy treatment for sputum retention, loss of volume or breathlessness
• select appropriate physiotherapy management options for managing sputum retention, loss of volume or breathlessness
• identify patients who need to be referred to the medical team for review, such as those who do not appear to be on optimum medication (e.g. steroids or bronchodilators) or those who require further investigations (e.g. chest X-rays or lung function tests)
• determine whether patients can be safely managed at home or whether they need to be in hospital (discharge planning for those in hospital, or admission decisions for patients at home)
• identify any support (e.g. social or medical) the patient may require in order to be discharged from hospital or remain at home
• identify and rate the patient’s functional ability and level of independence in activities of daily living
• identify the patient’s goals, e.g. in relation to improving mobility, function or social participation
• select appropriate physiotherapy management options for enabling functional ability and independence, and make referrals to other multidisciplinary team members
• facilitate the prescription of an exercise programme that is appropriate for the patient’s physical, psychological and social situation
• assess a patient’s suitability for pulmonary or cardiac rehabilitation
• assess a patient before and/or after intervention as an outcome measure for audit or research.
1.4 Assessment approaches
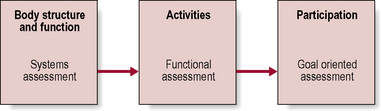
Physiotherapy assessment of the respiratory patient may be classified into three main approaches:
Goal-oriented assessment
These three approaches represent the three domains of ‘body structure and function’, ‘activity’ and ‘participation’ that have been identified in the International Classification of Functioning, Disability and Health, produced by the World Health Organization (see Further reading) (Fig. 1.4).
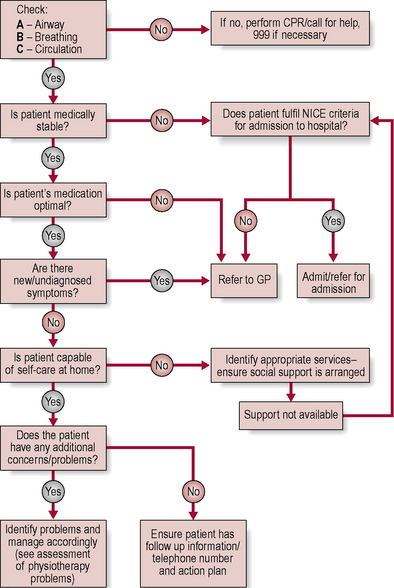
1.5 Assessment in the community
With an acutely ill patient, your role may involve making a decision about whether the patient needs admission to hospital or whether he or she requires urgent medical care in order to remain at home (Fig. 1.5). With more stable patients, your priority may be towards optimizing their mobility, function and quality of life to help them to achieve their personal goals and optimum potential. Assessment of an acute respiratory patient in the community setting requires analysis of medical, functional, environmental and social situations, which may be liable to change.
1.6 Clinical reasoning in respiratory care
At the end of your assessment you should ask yourself:
Problems related to respiration are frequently classified as one or more of the following:
Harden B., Cross J., Broad M., et al. Respiratory Physiotherapy: An On-call Survival Guide, 2nd edn. Edinburgh, UK: Churchill Livingstone; 2009.
National Institute for Health and Clinical Excellence. Management of Chronic Obstructive Pulmonary Disease in Adults in Primary and Secondary Care. Clinical Guideline 12. London, UK: NICE, 2010. Available at: http://www.nice.org.uk/nicemedia/live/13029/49399/49399.pdf/
World Health Organization. International Classification of Functioning, Disability and Health. Geneva, Switzerland: WHO; 2011. Available at: http://www.who.int/classifications/icf/en/