Complete agenesis: Complete absence of pancreatic neck, body, and tail, Santorini duct, and minor papilla
– Ventral pancreas (head and uncinate) appears normal
– MRCP: Visualization only of short ventral duct, with absence of accessory and dorsal duct system
Partial agenesis: Variable appearance of pancreatic body (depending on degree of agenesis), with small remnant Santorini duct and minor papilla
– Pancreas may appear short or truncated with normal pancreatic head and rounded upstream margin
• ERCP
Complete agenesis: Filling of short ventral duct without identifiable dorsal ducts or minor papilla
Partial agenesis: Main pancreatic duct is shortened, some dorsal ducts remain with filling of atretic Santorini duct
TOP DIFFERENTIAL DIAGNOSES
• Pancreatic ductal carcinoma
• Chronic pancreatitis (pseudoagenesis)
• Pancreatic divisum
• Pancreatic lipomatosis
• Post-traumatic pancreatic atrophy
PATHOLOGY
• Embryologic ventral bud forms inferior pancreatic head, uncinate process, and duct of Wirsung
• Embryologic dorsal bud forms pancreatic body, tail, superior head, Santorini duct, and minor papilla
• Agenesis of dorsal pancreas due to defect of dorsal bud
• Associated with polysplenia/heterotaxy syndrome and bowel malrotation
CLINICAL ISSUES
• Usually asymptomatic, but is associated with increased incidence of pancreatitis and diabetes
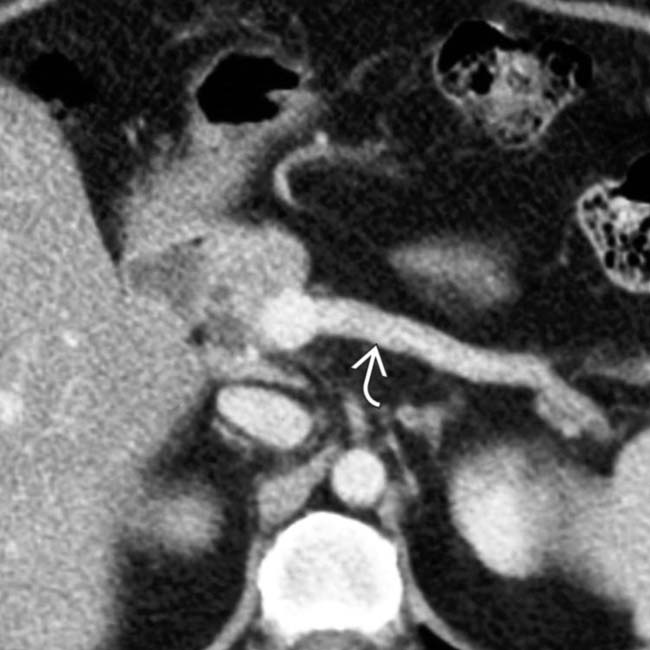
(Left) Axial CECT shows a normal-appearing pancreatic head , but neither body nor tail are present. This patient has congenital absence of the dorsal pancreas and has had at least 1 episode of acute pancreatitis.
(Right) ERCP shows filling of the ventral pancreatic duct within the head and uncinate process only, without filling of the ducts in the pancreatic body or tail, characteristic of agenesis of the dorsal pancreas. Note the normal tapering of the pancreatic duct and its side branches.
(Left) Axial CECT shows no pancreatic tissue or duct in the expected position of the body-tail segments. There should normally be pancreatic tissue along the anterior aspect of the splenic vein .
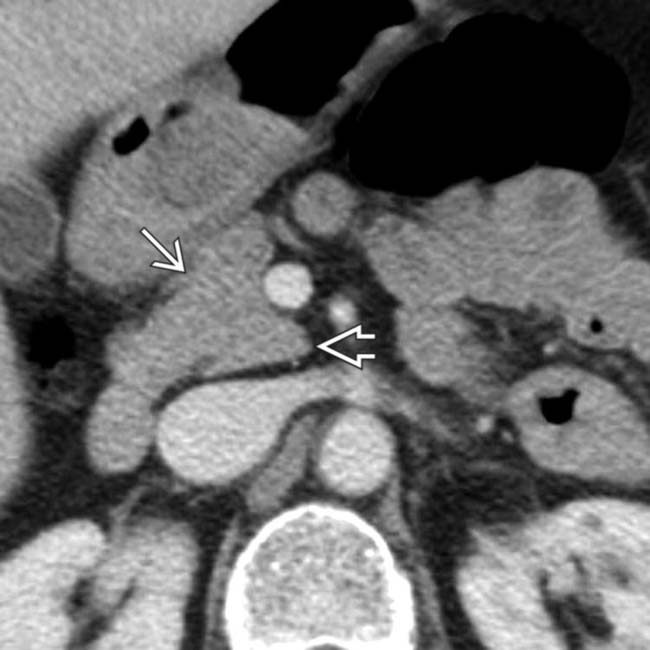
(Right) Axial CECT in a patient with polysplenia syndrome demonstrates partial agenesis of the dorsal pancreas. There is still a hypoplastic pancreatic body, which demonstrates a characteristic rounded margin , as well as complete absence of the pancreatic tail. Agenesis of the dorsal pancreas is associated with polysplenia.
Axial CECT shows the pancreatic head with focal calcifications, indicative of chronic pancreatitis. Glandular tissue and duct were completely absent in the body-tail segment.
ERCP shows filling of the pancreatic duct within the head and uncinate, but not in the absent pancreatic body. The pancreatic acini are filled with contrast due to forceful injection, which can induce pancreatitis.
Axial CECT demonstrates absence of the body and tail of the pancreas, which normally lie anteriorly along the course of the splenic vein . In the expected anatomic location normally occupied by the pancreatic body, there is only fat and a segment of small bowel . (Courtesy H. Harvin, MD.)
Axial CECT in the same patient demonstrates normal head of pancreas and uncinate process . (Courtesy H. Harvin, MD.)
 Partial agenesis: Variable appearance of pancreatic body (depending on degree of agenesis), with small remnant Santorini duct and minor papilla
Partial agenesis: Variable appearance of pancreatic body (depending on degree of agenesis), with small remnant Santorini duct and minor papilla



 , but neither body nor tail are present. This patient has congenital absence of the dorsal pancreas and has had at least 1 episode of acute pancreatitis.
, but neither body nor tail are present. This patient has congenital absence of the dorsal pancreas and has had at least 1 episode of acute pancreatitis.
 .
.
 , as well as complete absence of the pancreatic tail. Agenesis of the dorsal pancreas is associated with polysplenia.
, as well as complete absence of the pancreatic tail. Agenesis of the dorsal pancreas is associated with polysplenia.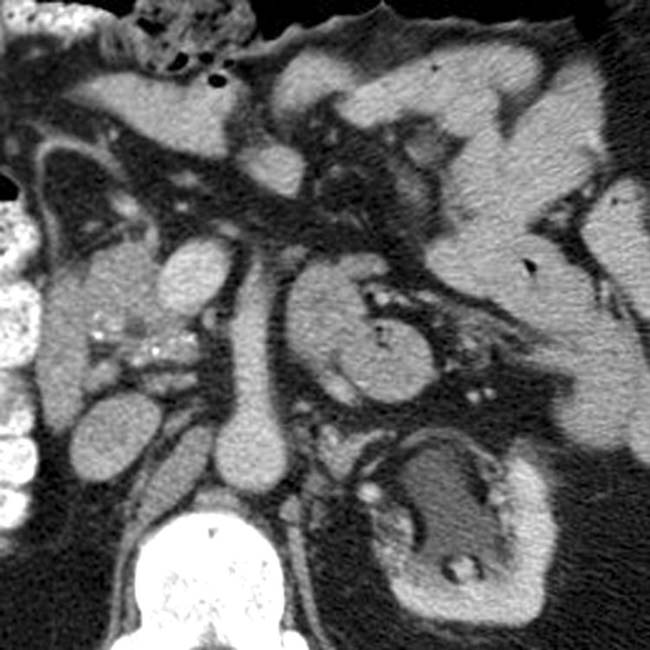

 within the head and uncinate, but not in the absent pancreatic body. The pancreatic acini are filled with contrast due to forceful injection, which can induce pancreatitis.
within the head and uncinate, but not in the absent pancreatic body. The pancreatic acini are filled with contrast due to forceful injection, which can induce pancreatitis.
 . In the expected anatomic location normally occupied by the pancreatic body, there is only fat and a segment of small bowel
. In the expected anatomic location normally occupied by the pancreatic body, there is only fat and a segment of small bowel  .
. 
 and uncinate process
and uncinate process  .
. 


