[level-membership-for-basic-science-category]47
Adrenocortical pathophysiology
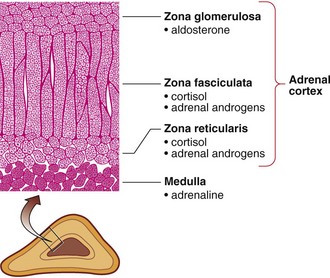
The hormones of the adrenal (suprarenal) glands are essential for survival. The adrenal cortex is the source of the two important steroid hormones, aldosterone and cortisol (Fig 47.1). The adrenal medulla is embryologically and histologically distinct from the cortex and is part of the sympathetic nervous system. Medullary cells synthesize, store and secrete adrenaline, along with noradrenaline and dopamine. The adrenal medullary hormones are discussed further on pages 136–137.
Cortisol
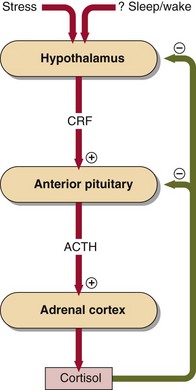
Cortisol is produced mainly in the zona fasciculata and in small quanities in the zona reticularis of the adrenal cortex, the end product of a cascade of hormones that make up the hypothalamic–pituitary–adrenocortical axis (Fig 47.2). Corticotrophin releasing hormone (CRH) is secreted by the hypothalamus under the influence of cerebral factors. Adrenocorticotrophic hormone (corticotrophin, or simply ACTH) is secreted by the anterior pituitary under the control of CRH to maintain the fascicular and reticular zones of the adrenal cortex and to stimulate the secretion of cortisol. Hypothalamic secretion of CRH and pituitary secretion of ACTH are modulated by cortisol in negative feedback loops.
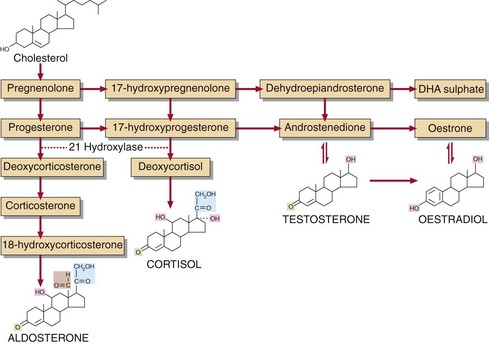
Adrenal cortex cells have many low-density lipoprotein receptors on their surface. This enables them to take up cholesterol rapidly, from which the adrenal steroid hormones are synthesized (Fig 47.3).
Aldosterone
Aldosterone is produced exclusively by the zona glomerulosa and is primarily controlled by the renin–angiotensin system (p. 15). The metabolic pathway for the synthesis of aldosterone utilizes many of the same enzymes involved in cortisol biosynthesis. The zona glomerulosa lacks the 17-hydroxylase enzyme and has the additional 18-hydroxylase and 18-hydroxysteroid dehydrogenase enzymes necessary for aldosterone synthesis.
 Clinical note
Clinical noteCongenital adrenal hyperplasia (CAH)
Because of the lack of cortisol, negative feedback to the pituitary is absent and ACTH secretion continues to drive steroid biosynthesis (Fig 47.3). Cortisol precursors are secreted in large amounts, their nature depending on which enzyme is lacking. The 21-hydroxylase is the deficient enzyme in 95% of cases of CAH. Here, large amounts of 17-hydroxyprogesterone are secreted. Elevated plasma concentrations are diagnostic as early as 2 days after birth. Increased stimulation of adrenal androgen production can cause virilization in baby girls, and precocious puberty in boys.
Relationship of adrenal cortex and medulla
Case history 37










[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]47
Adrenocortical pathophysiology
The hormones of the adrenal (suprarenal) glands are essential for survival. The adrenal cortex is the source of the two important steroid hormones, aldosterone and cortisol (Fig 47.1). The adrenal medulla is embryologically and histologically distinct from the cortex and is part of the sympathetic nervous system. Medullary cells synthesize, store and secrete adrenaline, along with noradrenaline and dopamine. The adrenal medullary hormones are discussed further on pages 136–137.
Cortisol
Cortisol is produced mainly in the zona fasciculata and in small quanities in the zona reticularis of the adrenal cortex, the end product of a cascade of hormones that make up the hypothalamic–pituitary–adrenocortical axis (Fig 47.2). Corticotrophin releasing hormone (CRH) is secreted by the hypothalamus under the influence of cerebral factors. Adrenocorticotrophic hormone (corticotrophin, or simply ACTH) is secreted by the anterior pituitary under the control of CRH to maintain the fascicular and reticular zones of the adrenal cortex and to stimulate the secretion of cortisol. Hypothalamic secretion of CRH and pituitary secretion of ACTH are modulated by cortisol in negative feedback loops.
Adrenal cortex cells have many low-density lipoprotein receptors on their surface. This enables them to take up cholesterol rapidly, from which the adrenal steroid hormones are synthesized (Fig 47.3).
