[level-membership-for-surgery-category]
CHAPTER 26 Adjustable gastric banding
Step 1. Surgical anatomy
♦ Adjustable gastric banding was first introduced in 1993. Initially the Lap-Band was the only band available, now we have two types: the Lap-Band System by Allergan Health (Figure 26-1) and the Realize Band by Ethicon Endo-Surgery (Figure 26-2).
♦ The first landmarks to establish are the location of the gastroesophageal junction and the angle of His. Often there will be a large gastroesophageal fat pad, which obscures the location of the gastroesophageal junction. The fat pad will need to be dissected away to identify the gastric serosa.
♦ Once the gastroesophageal junction is identified, then the presence of a hiatal hernia can be determined. If present, a hiatal hernia will need to be repaired to avoid future dysphagia and failure of the band.
♦ The hepatogastric ligament, which is part of the lesser omentum, connects the liver with the lesser curve of the stomach. It consists of a caudal flaccid portion known as the “pars flaccida,” which is usually transparent and contains no vessels. The right-sided dissection begins here, and there is usually no need to dissect in the more cranial portion of the hepatogastric ligament known as the “pars densa.” The pars densa should be avoided when possible because it contains the hepatic branch of the vagus nerve and an associated artery. If there is a replaced left hepatic artery, it will be located in this region and must be considered while dissecting in this region because it is often obscured by overlying fat.
♦ Once the pars flaccida is opened, the right diaphragmatic crus can be exposed. Proper identification of the right crus is critical to ensure safe dissection into the retrogastric space. Proper technique and placement of band will help the surgeon to avoid entering the lesser sac.
♦ A perigastric dissection occurs along the lesser curve of the stomach and requires meticulous tissue dissection. This approach may be utilized in cases when there is excess fat along the lesser curve, large accessory or replaced vessels, and poor visibility of the right crus.


Step 2. Preoperative considerations
Patient preparation
♦ The indications and contraindications for an adjustable gastric band are the same for all bariatric surgery patients.
♦ Preoperative assessment by a multidisciplinary team is required. The team should consist of the following: the bariatric surgeon, internists, endocrinologists, pulmonary staff, and cardiology staff, as well as consultation with nutritionists and psychological evaluation. The assessment is based on the patient’s individual needs.
♦ High body mass index (BMI) >50, advanced age, insulin resistance, and poor health are associated negative predictors but are not contraindications to banding procedures.
♦ Patients with a history of esophageal disorders or gastroesophageal reflux should undergo an upper GI contrast study, endoscopy and manometry. Any patient with a documented significant esophageal dysmotility disorder should not have a banding procedure.
♦ Preoperative weight loss is helpful in reducing injury to the liver, reducing operative time, and preparing the patient for postoperative dietary guidelines. Severely obese patients with BMI >50 are recommended to lose >10% of excess weight.
Equipment and instrumentation
♦ Three 5-mm bladeless trocars and one 15-mm bladeless trocar (the 15-mm trocar allows safe and easy passage of the band into the abdomen)
♦ Iron Intern with Nathanson liver retractor
♦ Foot-operated hook cautery for most cases (for patients with excess around the lesser curve and gastroesophageal junction, hand-operated ultrasonic shears are recommended)
Anesthesia
♦ DVT prophylaxis is recommended in all patients undergoing bariatric surgery. Consensus on mechanical versus pharmacologic versus combination has not been reached. No prospective randomized studies are available. I recommend using a combination of sequential compression devices and 5000 units of unfractionated heparin or 30 mg of low-molecular-weight heparin given subcutaneously 1 hour preoperatively and early ambulation postoperatively.
♦ Patients with history of DVT and Pulmonary embolism (PE) should be considered for prophylactic vena cava filter as well as patients with pulmonary hypertension, obesity hypoventilation syndrome, and a BMI >60.
♦ Antiemetics are recommended to reduce vomiting and potential postoperative band prolapse.
♦ Gastric decompression with NGT or calibration tube will allow easy visualization of anatomic landmarks.
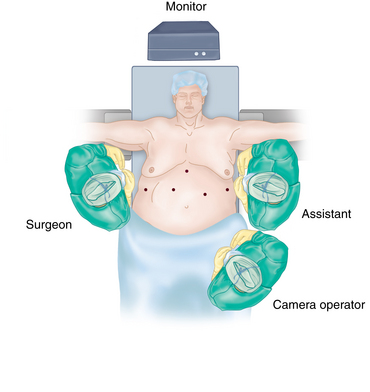
Room setup and patient positioning
♦ Place the patient in supine or split leg position with foot support, to allow patient to be placed in reverse Trendelenburg for the majority of the procedure.
♦ Protect all weight-bearing surfaces.
♦ The surgeon should be on the right side of the patient or between the patient’s legs and the assistant should be on the left side.
Step 3. Operative steps
Access and port placement
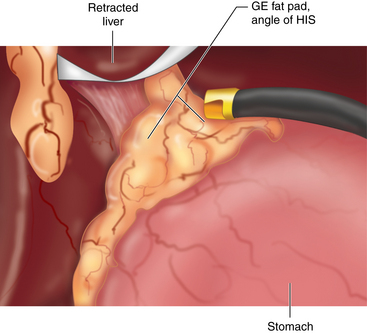
Exposure and dissection of angle of his
♦ The assistant sweeps greater curvature fat to expose the angle of His, while the surgeon retracts the anterior stomach wall caudally (Figure 26-4).
♦ Minimal dissection is needed to expose the anterior portion of the left crus.
♦ Sometimes, greater dissection is needed to identify the esophagogastric junction. The gastroesophageal fat pad may need to be removed to allow identification of the uppermost stomach, which is necessary for placement of the gastro-gastric sutures later in the procedure. It is best to perform these maneuvers at this stage, while the surgeon still has both hands available.
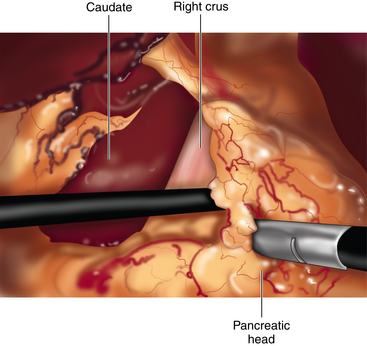
Exposure of right crus and creation of retrogastric tunnel
♦ Attention is moved to the right of the stomach for creation of the posterior tunnel.
♦ First, the hepatogastric ligament is opened using electrocautery or ultrasonic energy. Care is taken to avoid injury and bleeding from accessory vessels or a replaced left hepatic artery.
♦ Once the right crus is identified, we create a small opening at the junction of the right crus and the fatty tissue as far inferior on the crus as possible.
♦ The blunt-tipped dissecting instrument or grasper will be passed through the opening and into the retrogastric space. There is only a very short distance for the instrument to pass before it is seen exiting at the angle of His (Figure 26-5).
♦ The tip should pass through the retrogastric tissue without resistance. Any resistance should be worrisome and will require withdrawing the instrument a slight amount and redirecting the tip.
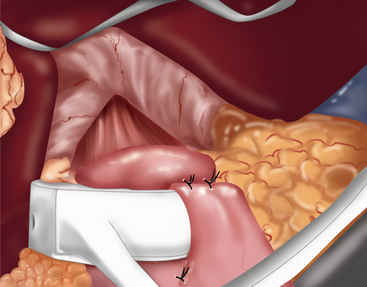
Band insertion and positioning
♦ The band is passed gently through the 15-mm port and directed toward the upper abdomen.
♦ The tubing of the Lap-Band or the suture of the Realize Band is placed in the tip of the retrogastric instrument. The band is pulled behind the stomach and pulled around the upper portion of the stomach. A 25-cc calibration tube can be used to help position the band if needed.
♦ The band should sit just below the gastroesophageal junction.
♦ Prior to buckling, it is important to assess the tightness of the band and remove any excess fat between the band and the stomach, then buckle the band.
♦ Then we remove the orogastric or calibration tube.
♦ The band is secured in place by anterior gastro-gastric plicating sutures. These nonabsorbable sutures can be placed in either interrupted or running fashion (Figure 26-6).
Subcutaneous port placement
♦ I have used several techniques over the years:
 The most basic method is to extend the incision of the 15-mm port, retract the incision open with narrow Deavers, and place nonabsorbable sutures using handheld instruments into the anterior rectus fascia.
The most basic method is to extend the incision of the 15-mm port, retract the incision open with narrow Deavers, and place nonabsorbable sutures using handheld instruments into the anterior rectus fascia.

♦ The transfascial suture passer technique is the technique I have routinely used for the past few years. This is the same concept that is applied when tacking the four quadrants of mesh in laparoscopic ventral hernia repair using the suture passer.




♦ The band tubing is pulled out through the 15-mm fascial defect as the port is removed.
♦ The liver retractor is removed, pneumoperitoneum is released, and all ports are removed.
♦ The subcutaneous port is attached to the tubing, and the excess tubing is tucked into the abdomen. The subcutaneous port is then parachuted into the wound and secured to the fascia.
♦ Fascial defects may need to be closed if there is little subcutaneous tissue. Generally, the fascial defect created by the bladeless devices do not require closure especially when located high in the abdomen at the falciform ligament..
Step 4. Postoperative care
♦ After surgery, we obtain an esophagram to rule out obstruction/leak and provide a baseline assessment.
♦ Start clear liquids, and advance to puree for 3 weeks.
♦ Begin solids at 3 to 4 weeks.
♦ Office-based adjustments are started 5 weeks after surgery.
♦ Set a weight-loss goal of 1 to 3 pounds per week.
♦ Follow up every month or as needed with nutritional counseling.
Step 5. Pearls and pitfalls
♦ Gastric perforation related to dissection of angle of His, and passing dissector posterior to stomach.
♦ Splenic injury caused by excessive traction on greater curvature fat.
♦ Liver injury resulting from a fatty liver.
♦ Improper band placement—too high or too low.
♦ Avoid postoperative band obstruction by dissecting excessive perigastric fat, removing the gastroesophageal fat pad, and choosing the appropriate size band.
♦ Port site infection can be reduced by following proper antiseptic techniques when performing adjustments. If port site infection occurs, a trial of oral antibiotics is recommended. If the patient does not improve, it will be necessary to rule out band erosion with upper endoscopy.
♦ Band prolapse occurs approximately 5% to 10% of the time and requires reoperation to reposition or replace band.
♦ Band erosion occurs in 1% to 2% of patients. Avoid excessive traction on stomach and do not cover buckle area of band with stomach to reduce erosion. If erosion is diagnosed, the band will have to be removed.
♦ Esophageal dilatation occurs approximately 5% of the time, because of over-tightening of the band and poor follow-up. It is recommended to deflate the band for 1 month and repeat the esophagram. Once the esophagus diameter has improved, the surgeon may readjust.
Belachew M, Legrand M, Vincenti VV, et al. Laparoscopic placement of adjustable silicone gastric band in the treatment of morbid obesity: how to do it. Obes Surg. 1995;5;1:66-70.
O’Brien PE, Dixon JB. Laparoscopic adjustable gastric banding. In: Inabnet WB, DeMaria EJ, Ikramuddin S, editors. Laparoscopic Bariatric Surgery. Melbourne, Australia: Lippincott Williams & Wilkins; 2005:75-84.
Vertruyen M. Experience with Lap-Band System up to 7 years. Obes Surg. 2002;12(4):569-572.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
CHAPTER 26 Adjustable gastric banding
Step 1. Surgical anatomy
♦ Adjustable gastric banding was first introduced in 1993. Initially the Lap-Band was the only band available, now we have two types: the Lap-Band System by Allergan Health (Figure 26-1) and the Realize Band by Ethicon Endo-Surgery (Figure 26-2).
♦ The first landmarks to establish are the location of the gastroesophageal junction and the angle of His. Often there will be a large gastroesophageal fat pad, which obscures the location of the gastroesophageal junction. The fat pad will need to be dissected away to identify the gastric serosa.
♦ Once the gastroesophageal junction is identified, then the presence of a hiatal hernia can be determined. If present, a hiatal hernia will need to be repaired to avoid future dysphagia and failure of the band.
♦ The hepatogastric ligament, which is part of the lesser omentum, connects the liver with the lesser curve of the stomach. It consists of a caudal flaccid portion known as the “pars flaccida,” which is usually transparent and contains no vessels. The right-sided dissection begins here, and there is usually no need to dissect in the more cranial portion of the hepatogastric ligament known as the “pars densa.” The pars densa should be avoided when possible because it contains the hepatic branch of the vagus nerve and an associated artery. If there is a replaced left hepatic artery, it will be located in this region and must be considered while dissecting in this region because it is often obscured by overlying fat.
♦ Once the pars flaccida is opened, the right diaphragmatic crus can be exposed. Proper identification of the right crus is critical to ensure safe dissection into the retrogastric space. Proper technique and placement of band will help the surgeon to avoid entering the lesser sac.
♦ A perigastric dissection occurs along the lesser curve of the stomach and requires meticulous tissue dissection. This approach may be utilized in cases when there is excess fat along the lesser curve, large accessory or replaced vessels, and poor visibility of the right crus.
Step 2. Preoperative considerations
Patient preparation
♦ The indications and contraindications for an adjustable gastric band are the same for all bariatric surgery patients.
♦ Preoperative assessment by a multidisciplinary team is required. The team should consist of the following: the bariatric surgeon, internists, endocrinologists, pulmonary staff, and cardiology staff, as well as consultation with nutritionists and psychological evaluation. The assessment is based on the patient’s individual needs.
♦ High body mass index (BMI) >50, advanced age, insulin resistance, and poor health are associated negative predictors but are not contraindications to banding procedures.
♦ Patients with a history of esophageal disorders or gastroesophageal reflux should undergo an upper GI contrast study, endoscopy and manometry. Any patient with a documented significant esophageal dysmotility disorder should not have a banding procedure.
♦ Preoperative weight loss is helpful in reducing injury to the liver, reducing operative time, and preparing the patient for postoperative dietary guidelines. Severely obese patients with BMI >50 are recommended to lose >10% of excess weight.
Equipment and instrumentation
♦ Three 5-mm bladeless trocars and one 15-mm bladeless trocar (the 15-mm trocar allows safe and easy passage of the band into the abdomen)
♦ Iron Intern with Nathanson liver retractor
♦ Foot-operated hook cautery for most cases (for patients with excess around the lesser curve and gastroesophageal junction, hand-operated ultrasonic shears are recommended)
Anesthesia
♦ DVT prophylaxis is recommended in all patients undergoing bariatric surgery. Consensus on mechanical versus pharmacologic versus combination has not been reached. No prospective randomized studies are available. I recommend using a combination of sequential compression devices and 5000 units of unfractionated heparin or 30 mg of low-molecular-weight heparin given subcutaneously 1 hour preoperatively and early ambulation postoperatively.
♦ Patients with history of DVT and Pulmonary embolism (PE) should be considered for prophylactic vena cava filter as well as patients with pulmonary hypertension, obesity hypoventilation syndrome, and a BMI >60.
[/not-level-membership-for-surgery-category]
