CHAPTER 35 Adjustable Breast Implants for Asymmetry and Ptosis
Summary/Key Points
Patient Selection
Fortunately, today’s surgeons have adjustable implants available to them. Adjustable implants offer the surgeon the ability to select the implant based primarily on base diameter and then alter the volume and projection intraoperatively or postoperatively. Adjustable implants include single-lumen saline, double-lumen saline-gel, and adjustable gel. These implants offer considerable benefit to surgeons by simplifying implant selection and allowing for subsequent alteration for the treatment of asymmetry noted here.1–3
Indications
Asymmetry
Debate continues about the incidence of breast asymmetry. One estimate suggests that asymmetry presents in 80% of the population, to the trained eye, and increases to 100% when measured with the appropriate tools.4 In this line of thought, surgeons often counsel patients that some degree of asymmetry is an inevitable. Moreover, attempts to correct the asymmetry after the first operation often lead to further complications. Use of the adjustable implant offers the surgeon the ability to more effectively manage asymmetry correction.
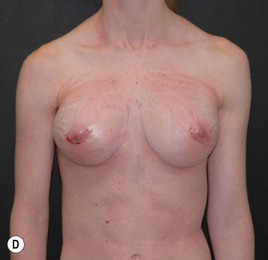
Some physicians may argue that asymmetry cannot be fully corrected. We would argue that this argument may be valid when using fixed volume implants. However, with adjustable implants asymmetry can be accurately corrected. The adjustable implant can be increased or decreased post implantation, leading to high degrees of correction of asymmetry Figs 35.1–35.5 illustrate the presence of asymmetry and scoliosis, followed by installation of an adjustable implant, adjustment of volume, after surgery, and satisfactory correction of the breast defects.







































Mastopexy-augmentation
If breast elevation is asymmetrical or insufficient, adding saline can cause further elevation and thus improve symmetry. In cases of breast base constriction such as tubular breast deformity, overexpansion and volume reduction can be of benefit in improving the shape of the breast.5–10
Figures 35.3 and 35.4 illustrate preoperative presence of breast ptosis and asymmetry, followed by successful mastopexy and implantation with an adjustable implant.
Operative Technique
Types of adjustable implants
Single-lumen saline implant (Spectrum®)
The adjustable saline implant functions exactly like a normal saline implant, with the added advantage of volume increase and decrease capabilities. The Spectrum valve has a significantly lower leakage rate compared to the diaphragm valve in the regular saline implant.7
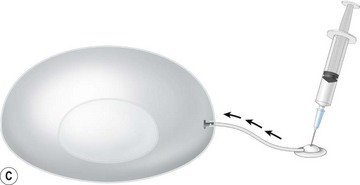
Perioperative versus postoperative volume adjustment. Some physicians prefer to adjust the volume of the implant at the time of surgery. Postoperative adjustability has the added advantage of reducing implant rippling, with a saline adjustable implant, should the surgeon wish to delay filling the implant until after surgical procedures have been completed (Fig. 35.6).




Ordinarily, the Spectrum is placed submuscularly. The implant can also function as a temporary expander, to decrease capsular contracture. It can be placed in the patient virtually empty, for example, when the surgeon is treating resistant synmastia (absence of cleavage). It may be placed above the muscle to expand and shape of the subglandular pocket, for example with a short inframammary crease or with a case of severe asymmetry, and then later replaced with a gel implant if necessary.6
Double-lumen saline-gel implant (Becker-Mentor)
Model implant names of the double-lumen saline-gel implant are as follows: Becker 50/50, Becker 25/75 and the Contour Profile (CP) Becker implants. The Becker 50/50 is composed of 50% gel in the outer chamber and 50% saline in the inner chamber. The Becker 25/75 is a double-lumen implant with 25% gel in the outer chamber and 75% saline in the inner chamber. The CP Becker is an anatomically shaped implant with 35% gel in the outer chamber and 65% saline in the inner chamber. Figure 35.7A, B and also Figure 35.8F show these three double-lumen implants.







Adjustable gel implant (Mentor Spectra Becker)
The ability to alter implant size and projection at the time of surgery eliminates the need to discard an implant that does not have the correct dimension. In addition, in the event that the desired gel implant is not available, the Spectra adjustable gel implant can be an ideal alternative because of its flexibility. Figure 35.8 illustrates various gel volumes in the Spectra.
Technique
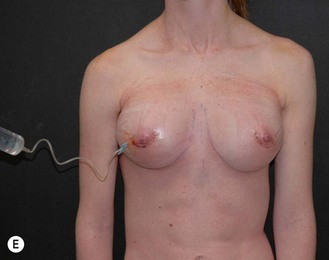
The volume of the adjustable implant may be fine tuned at the time of surgery and the fill tube pulled on the operating table. Alternatively, the desired amount of saline may be added at the time of surgery and postoperative adjustment made via the injection dome. Jackson Pratt drains are routinely used. The injection dome may be exteriorized or buried.11,12
Exteriorized injection dome
The injection dome is exteriorized by attaching the fill tube to a trochar and bringing it out through a long subcutaneous tunnel. The fill tube is then attached to the injection port or to an Interlimit injection site (Baxter Deerfield, IL). The port can be exteriorized for 7–10 days, after which it is removed. Although surgeons are always mindful of infection control, they can have confidence in use of the exteriorized injection dome. In over 100 cases, no retrograde infections have been reported.13,14
Buried injection dome
The domes are buried in cases of severe asymmetry, in Poland’s syndrome, or with tubular breasts where postoperative expansion will likely be necessary. Burying the injection domes has an obvious advantage in mastopexy augmentation, where concern about skin flaps is a consideration, in revision surgery, and in patients with major concerns about size and symmetry. Figure 35.4 shows implantation and removal of injection dome.
Figure 35.5J, K and Figure 35.5H show incision site for removal of injection dome after treatment of defect of left breast.
Pitfalls and How to Correct
Postoperative Care
Postoperative filling is done using a 23-gauge butterfly needle. Using sterile technique, 25–100 ml of saline may be added. Implants may be placed underfilled if necessary. However, the filling volumes recommended by the manufacturer are quite limiting. In our practice, we have added a paragraph to our consent form stating that exceeding these volumes may be necessary. Implants have been temporarily overfilled for several weeks and even left at a volume above the recommended when necessary. In a study done on the Smooth Spectrum® implant, there was no increased leakage in overfilled implants. In fact, the only leakage found was in an under-filled implant. Exteriorized injection domes are removed a few days after surgery (up to 10 days). Buried injection domes are removed 3–12 months after surgery. The patient is placed on prophylactic antibiotics and the injection dome removed under local anesthetic. The original incision is usually used for access.9,10
Figure 35.3A–H shows deliberate overinflation of an adjustable implant for temporary correction, followed by insertion of silicone gel implants.
1 Becker H. Augmentation mastopexy using adjustable implants with external injection domes. Aesth Surg J. 2006;26(4):736-740.
2 Becker H. Use of the adjustable Spectrum implant in aesthetic breast surgery. Innovations Plast Surg. 2005;1:64-81.
3 Becker H. Breast augmentation using the Spectrum implant with exteriorized injection domes. Plast Reconstr Surg. 2004;111(1):1617-1620.
4 Allergan Academy. ASAPS, 2008 (April, San Diego, CA).
5 Becker H. The correction of breast ptosis with the expander mammary prosthesis. Ann Plast Surg. 1990;24(6):489-497.
6 Becker H. Expansion augmentation. Clin Plast Surg. 1988;15(4):587-593.
7 Becker H, Carlisle H, Kay J. Filling implants beyond the manufacturers recommended fill volume. Aesth Plast Surg. 2008;32(3):432-441.
8 Becker H. Subareolar mastopexy: update. Aesth Surg J. 2003;September/October:357-363.
9 Persoff M, Becker H. Choosing size for an augmentation mammoplasty. Plast Reconstr Surg. 2002;109(1):397.
10 Becker H. The dermal overlap subareolar mastopexy: a preliminary report. Aesth Surg J. 2001;September/October:423-427.
11 Becker H. Adjustable breast implants provide postoperative versatility. Aesth Surg J. 2000;July/August:332-334.
12 Becker H. What is adequate fill? Implications in breast implant surgery. Plast Reconstr Surg. 1997;99(2):599.
13 Becker H. Breast expansion augmentation; the expander mammary implant for breast reconstruction. In: Rolf E Nordstrom MD, editor. Tissue expansion. Newton, Mass: Butterworth-Heinemann, 1996.
14 Becker H. How they do it (breast augmentation). Proc Plast Reconstr Surg. (June):1991.