[level-membership-for-basic-science-category]18
Acute renal failure
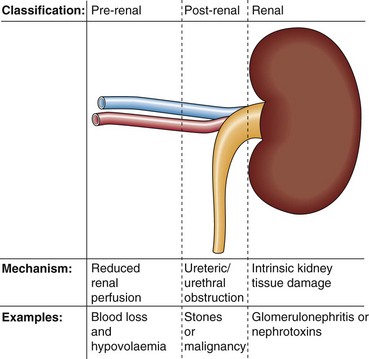
Aetiology



Diagnosis



Biochemical findings in pre-renal uraemia include the following:
 Serum urea and creatinine are increased. Urea is increased disproportionately more than creatinine because of its reabsorption by the tubular cells, particularly at low urine flow rates. This leads to a relatively higher serum urea concentration than creatinine, which is not so readily reabsorbed.
Serum urea and creatinine are increased. Urea is increased disproportionately more than creatinine because of its reabsorption by the tubular cells, particularly at low urine flow rates. This leads to a relatively higher serum urea concentration than creatinine, which is not so readily reabsorbed.
 Metabolic acidosis: because of the inability of the kidney to excrete hydrogen ions.
Metabolic acidosis: because of the inability of the kidney to excrete hydrogen ions.
 Hyperkalaemia: because of the decreased glomerular filtration rate and acidosis.
Hyperkalaemia: because of the decreased glomerular filtration rate and acidosis.



Acute tubular necrosis
 acute blood loss in severe trauma
acute blood loss in severe trauma

 specific renal disease, such as glomerulonephritis
specific renal disease, such as glomerulonephritis
 nephrotoxins, such as the aminoglycosides, analgesics or herbal toxins.
nephrotoxins, such as the aminoglycosides, analgesics or herbal toxins.
It may be difficult to decide the reason for a patient’s oliguria. The biochemical features that distinguish pre-renal uraemia from intrinsic renal damage are shown in Table 18.1.
Table 18.1
Biochemical features in the differential diagnosis of the oliguric patient
| Biochemical feature | Pre-renal failure | Intrinsic renal damage |
| Urine sodium | <20 mmol/L | >40 mmol/L |
| Urine/serum urea | >10 : 1 | <3 : 1 |
| Urine/plasma osmolality | >1.5 : 1 | <1.1 : 1 |
Management
Important issues in the management of the patient with ARF include:




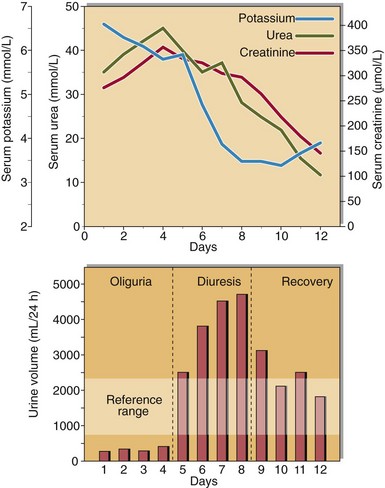
Recovery
There may be three distinct phases in the resolving clinical course of a patient with acute renal failure (Fig 18.2). An initial oliguric phase, where glomerular impairment predominates, is followed by a diuretic phase when urine output is high, as glomerular function slowly improves but tubular function remains impaired. During a recovery phase, complete renal function may return. Careful clinical and biochemical monitoring is necessary throughout the course of the patient’s illness.
 Clinical note
Clinical noteCase history 13
A male, aged 50, presented with pyrexia. He was clinically dehydrated and oliguric.

Acute renal failure






[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]18
Acute renal failure
Aetiology
Diagnosis
Biochemical findings in pre-renal uraemia include the following:
Serum urea and creatinine are increased. Urea is increased disproportionately more than creatinine because of its reabsorption by the tubular cells, particularly at low urine flow rates. This leads to a relatively higher serum urea concentration than creatinine, which is not so readily reabsorbed.
Metabolic acidosis: because of the inability of the kidney to excrete hydrogen ions.
[/not-level-membership-for-basic-science-category]
