CHAPTER 69 Acute Pericarditis
Acute pericarditis may result in fibrinous exudate, pericardial effusion, or cardiac tamponade. Various systemic diseases may result in acute pericarditis or pericardial effusion (see Chapter 68). In many cases, the cause of the acute pericarditis is unknown, however.
PREVALENCE AND EPIDEMIOLOGY
The true prevalence of acute pericarditis is unknown, but it may account for 1% of all emergency department visits for chest pain.1
ETIOLOGY AND PATHOPHYSIOLOGY
There are many causes of acute pericarditis (Table 69-1).2–6 The specific etiology is often unknown, thereby resulting in the diagnosis of idiopathic pericarditis. The use of a systematic approach to the diagnosis of the cause of acute pericarditis, including a detailed history, blood cultures, antibody testing, and viral testing, can reduce the number of “idiopathic” diagnoses.7 Viral infection is the most common cause of acute pericarditis in the United States, and is probably the etiology in patients with idiopathic pericarditis.8,9 The most common viral agents causing acute pericarditis are coxsackievirus group B and echovirus.8 Viral pericarditis is usually preceded by upper respiratory infection symptoms, and typically is a self-limited disease that can be diagnosed by serologic testing of antiviral titers. Numerous systemic diseases can also result in acute pericarditis and pericardial effusion. These diseases are discussed in Chapter 70. It is difficult to distinguish cases of acute pericarditis from cases of pericardial effusion in the literature because the presence of pericardial fluid is sometimes seen as an indicator of the presence of pericarditis.
MANIFESTATIONS OF DISEASE
Clinical Presentation
On physical examination, the patient typically appears distressed and often is leaning forward when sitting because this position helps to alleviate the pain. Fever may be present and typically follows the onset of pain. In 85% of patients, a triphasic pericardial friction rub, often characterized as the sound of leather squeaking against leather, is heard on auscultation, although this finding may be intermittent. The intensity of the rub can vary with the position of the patient. Characteristic ECG changes also are associated with acute pericarditis. Early in the disease, there is ST segment elevation in a nonanatomic distribution. The triad of characteristic pain, pericardial friction rub, and characteristic ECG changes is diagnostic of acute pericarditis. Laboratory abnormalities associated with acute viral or idiopathic pericarditis include elevation of the erythrocyte sedimentation rate and C-reactive protein, and early leukocytosis followed by development of lymphocytosis. Serum enzymes, such as creatine phosphokinase, and troponin levels may be elevated in patients with acute pericarditis because of a concomitant superficial myocarditis (also called myopericarditis).10
Imaging Techniques and Findings
Ultrasonography
Echocardiography may be performed to assess for the presence of pericardial effusion, to assess for evidence of cardiac tamponade, or to establish a baseline appearance of the pericardial space. The echocardiographic findings of acute pericarditis include a normal examination, pericardial thickening with or without pericardial effusion, and pericardial effusion without pericardial thickening.11 Depending on the echocardiographic findings, assessment can be made for tamponade or constrictive physiology.
Computed Tomography
Contrast-enhanced CT scans may be performed in patients in whom the clinical presentation is unclear or to exclude other potential causes of chest pain. Typical findings of acute pericarditis on CT scans include enhancement of smooth, uniformly thickened pericardium and pericardial effusion (Fig. 69-1).12
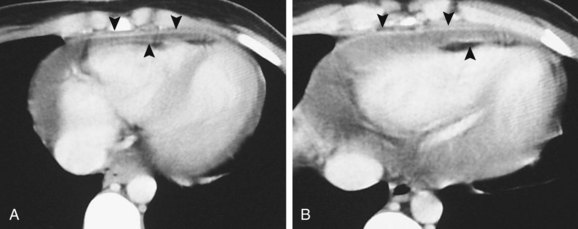
 FIGURE 69-1
FIGURE 69-1DIFFERENTIAL DIAGNOSIS
Imaging Findings
Pericardial thickening in patients with constrictive pericarditis may be calcified and is often irregular. Early enhancement of the pericardium is seen in patients with acute pericarditis studied with CT or MRI. If perfusion MRI is performed, there is typically delayed enhancement of the pericardium in patients with constrictive pericarditis, a feature that is absent in patients with acute pericarditis. The typical morphologic changes associated with constrictive pericarditis (see Chapter 70) are absent in patients with acute pericarditis.
TREATMENT OPTIONS
Medical
For viral or idiopathic pericarditis, ibuprofen is the preferred nonsteroidal anti-inflammatory drug. It is used to prevent recurrence of pericarditis.2,10,13 Antibiotic therapy is indicated when specific organisms are cultured.
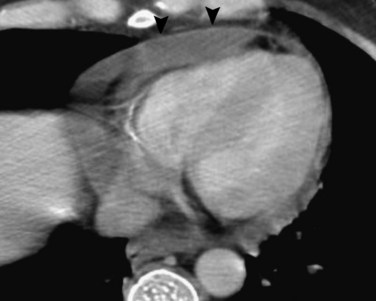
 FIGURE 69-2
FIGURE 69-2


1 Zayas R, Anguita M, Torres F, et al. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995;75:378-382.
2 Lange RA, Hillis LD. Acute pericarditis. N Engl J Med. 2004;351:2195-2202.
3 Spodick DH. Pericarditis in systemic diseases. Cardiol Clin. 1990;8:709-716.
4 Troughton RW, Asher CR, Klein AL. Pericarditis. Lancet. 2004;363:712-727.
5 Lorbar M, Spodick DH. “Idiopathic” pericarditis—the clinician’s challenge (nothing is idiopathic). Int J Clin Pract. 2007;91:138-142.
6 Ariyarajah V, Spodick DH. Acute pericarditis: diagnostic cues and common electrocardiographic manifestations. Cardiol Rev. 2007;15:24-30.
7 Levy PY, Corey R, Berger P, et al. Etiologic diagnosis of 204 pericardial effusions. Medicine (Baltimore). 2003;82:385-391.
8 Shabetai R. Acute pericarditis. Cardiol Clin. 1990;8:639-644.
9 Little WC, Freeman GL. Pericardial disease. Circulation. 2006;113:1622-1632.
10 Spodick DH. Acute pericarditis: current concepts and practice. JAMA. 2003;289:1150-1153.
11 Otto CM. Pericardial disease: two-dimensional echocardiographic and Doppler findings. In: Otto CM, editor. Textbook of Clinical Echocardiography. Philadelphia: Saunders; 2000:213-228.
12 Rienmüller R, Gröll R, Lipton MJ. CT and MR imaging of pericardial disease. Radiol Clin North Am. 2004;42:587-601.
13 Maisch B, Seferovic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary: the Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Eur Heart J. 2004;25:587-610.
