[level-membership-for-surgery-category]
Problem 22 Acute back pain in a 75-year-old man
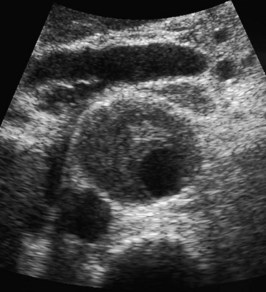
The patient recently had an abdominal ultrasound for his urinary frequency (Figures 22.1 and 22.2).

The ultrasound findings confirm your clinical suspicions.
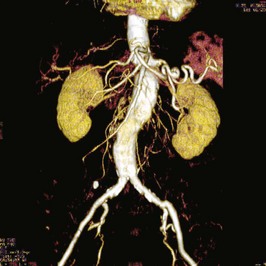
As this patient is haemodynamically stable, a further investigation is performed expeditiously. Two of the images are shown (Figures 22.3 and 22.4).

Q.5
What type of images are these and what do they show? How do these findings affect your management?
The patient makes an uneventful recovery and is home 10 days after the procedure.
Answers
A.2 The ultrasound shows a large fusiform abdominal aortic aneurysm. The image in Figure 22.1 shows the aneurysm in transverse section and in Figure 22.2 the aorta in longitudinal view. Some thrombus is shown in the posterior wall. The measurement of aneurysm size is taken on the transverse image and is the maximum anteroposterior or transverse diameter. The length of the aneurysm is not important from a management point of view.
A.5 Figure 22.3 shows a standard transverse cut through the aneurysm sac. Contrast has been administered and the non-enhancing contents of the aneurysm sac represent laminated thrombus. It is these images which provide the surgeon with vital information regarding the presence or absence of a leak. This shows a 5.8 cm abdominal aortic aneurysm which had not leaked. The pain is presumably due to expansion and stretching of the aneurysm.
Figure 22.4 is a spiral CT angiogram reconstruction. The reconstruction gives the surgeon useful information regarding patency/stenoses of renal and iliac arteries, vessel tortuosity and relationship of the aneurysm to the renal arteries. The renal arteries are patent and the iliac vessels are not aneurysmal.
Revision Points
Abdominal Aortic Aneurysms (AAA)
Pathology
Management
Symons N.R, Gibbs R.G. The management of abdominal aortic aneurysms. British Journal of Hospital Medicine. 2009;70:566-571. A review of current management
United Kingdom Small Aneurysm Trial Participants. Long-term outcomes of immediate repair compared with surveillance of small abdominal aortic aneurysms. New England Journal of Medicine, 346. 2002:1445-1452. www.NEJM.com.
www.scvir.org/patient/aaa/. A website from the Society for Cardiovascular and Interventional Radiology. Patient directed but with good information about endoluminal treatments
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Problem 22 Acute back pain in a 75-year-old man
The patient recently had an abdominal ultrasound for his urinary frequency (Figures 22.1 and 22.2).
The ultrasound findings confirm your clinical suspicions.
As this patient is haemodynamically stable, a further investigation is performed expeditiously. Two of the images are shown (Figures 22.3 and 22.4).
Q.5
What type of images are these and what do they show? How do these findings affect your management?
[/not-level-membership-for-surgery-category]
