127
Actinic keratosis

Multiple hypertrophic actinic keratosis scattered diffusely over the dorsal hand. Some of the thicker actinic keratoses may be difficult to distinguish from squamous cell carcinoma.
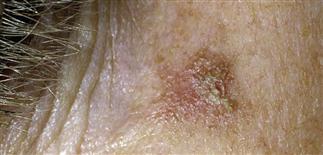
Single 3–5-mm actinic keratosis with thick hypertrophic scale centrally, that may be palpable, and rough surrounding pink changes peripherally.

Actinic keratosis may accumulate a dense scale on the surface and become a cutaneous horn. These lesions require excision.

Diffuse actinic damage of the lower vermillion lip with a blunting of the junction between the red vermillion border and the cutaneous lip with advanced actinic damage and early erosive changes.
DESCRIPTION
Common, persistent, keratotic lesions with malignant potential. Most commonly on sun-exposed areas of fair-skinned elderly patients, with significant sun exposure. Over time, actinic keratoses evolve into squamous cell carcinoma (SCC) or basal cell carcinoma (BCC).
HISTORY
• Result of years of cumulative sun exposure and keratinocyte damage. • Progressively more common after age 40. • Spontaneous regression occurs. • About 10–20% of actinic keratoses (AKs) progress to SCC or BCC over several years. Multiple AKs indicates a history of significant sun exposure and increased risk of skin cancer.
PHYSICAL FINDINGS
• AKs are found along with other signs of chronic sun exposure, such as uneven pigmentation, atrophy or thinning, telangiectasias. Predominantly on face, head, neck, dorsal hands. • Initially present as poorly defined area of redness or telangiectasia. Over time, become more defined and develop thin, adherent, yellowish or transparent scale. • Easier to detect by palpation than by observation. • Scale becomes progressively thicker, yellow. Retained scale may form elongated keratinous structure or cutaneous horn. Such advanced lesions may be difficult to distinguish from squamous cell carcinoma without biopsy. • Spreading pigmented AK: AKs with fine reticulated pigmentation. May mimic solar lentigo, melanoma in situ. • Hypertrophic AK: firm, thick, elevated keratotic AK that may indicated progression to true SCC. More aggressive treatment required. Actinic cheilitis: sun-induced keratinocyte atypia, lower lip. Focal crusting, scaling, along with blurring of vermilion border—appears whitish, gray. Actinic lesions in this location can be subtle clinically, behave aggressively. • AKs of lower legs frequently multiple, hyperkeratotic, distributed over large area. Numerous lesions may form on dorsal hand.
TREATMENT
• Patients with multiple AKs require frequent follow-up. • Visible or detectable lesions represent fraction of total number of atypical keratinocytes present. • Most of atypia scattered within sun-damaged skin and below level of clinical detection. • Multiple AKs indicates that patients are much more likely to develop more lesions with time. • Application of liquid nitrogen (cryotherapy) to solitary, superficial lesions is most common removal method. • Patients with significant photodamage, multiple and recurrent lesions, present difficult treatment problems. • Topical 5-fluorouracil 5% useful in reducing number of atypical keratinocytes. Erythema will appear if AKs present. Followed by burning and oozing. Treatment may be stopped before completing 3-week course if inflammation too intense. • Diclofenac sodium (Solaraze) gel, imiquimod (Aldara) 5% cream, and photodynamic therapy are other methods used to treat an entire area of photodamaged skin, multiple AKs and reduce skin cancer risk. • All therapies have a potential risk of post-procedure hypopigmentation, scar formation, especially in darker-skinned patients. Clearly explain this to patient before treatment. • Carbon dioxide laser vermillionectomy and topical 5-fluorouracil 5% cream possible treatments for actinic cheilitis. • Squamous cell carcinoma can develop from AK, especially with thicker lesions, lesions non-responsive to treatment, and lower lip lesions. Consider biopsy to look for invasive SCC in patients who do not respond appropriately to treatment and in recurrent or hypertrophic AKs.






