Acid–base disorders
diagnosis and management
Specimens for blood gas analysis
If the [H+] and the PCO2 are known, the bicarbonate can be calculated. Indeed, blood gas analysers (Fig 24.1) are programmed to provide this on all samples, as the ‘standard bicarbonate’ i.e. under standard conditions. Other parameters usually included are the PO2, and the base excess, another way of assessing the metabolic component.
Interpreting results
The most important information available for the interpretation and classification of an acid-base disorder is provided by the patient’s clinical history. The predicted compensatory responses in [HCO3–] or PCO2 when [H+] changes as a result of primary acid–base disorders are shown in Table 24.1.
Table 24.1
Primary acid–base disorders and compensatory responses
| Primary disorder | Compensatory response |
| ↑PCO2 (Respiratory acidosis) | ↑HCO3– |
| ↓PCO2 (Respiratory alkalosis) | ↓HCO3– |
| ↓HCO3– (Metabolic acidosis) | ↓PCO2 |
| ↑HCO3– (Metabolic alkalosis) | ↑PCO2 |
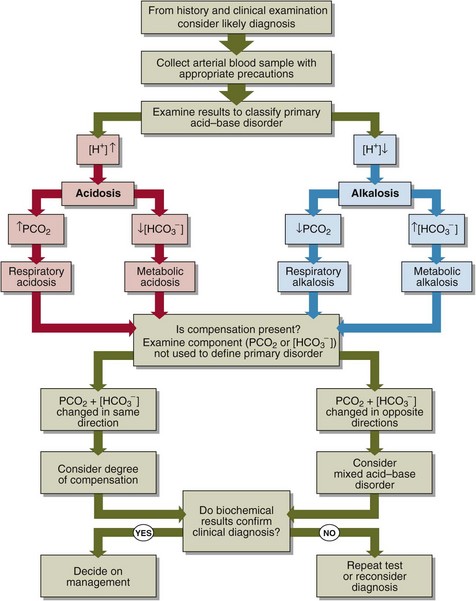
A practical approach to the interpretation of blood gas results is shown in Figure 24.2. The steps in classifying the acid–base disorder are:





Clinical cases
The above practical advice is best illustrated by four case examples.




Management of acid–base disorders
 fluid therapy and insulin in diabetic ketoacidosis
fluid therapy and insulin in diabetic ketoacidosis

 improvement of GFR by restoring blood volume in a patient with acute blood loss.
improvement of GFR by restoring blood volume in a patient with acute blood loss.
 Clinical note
Clinical noteCase history 18






