Chapter 1 Abdominal Wall Anatomy and Vascular Supply
1 Clinical Anatomy
1 Overview
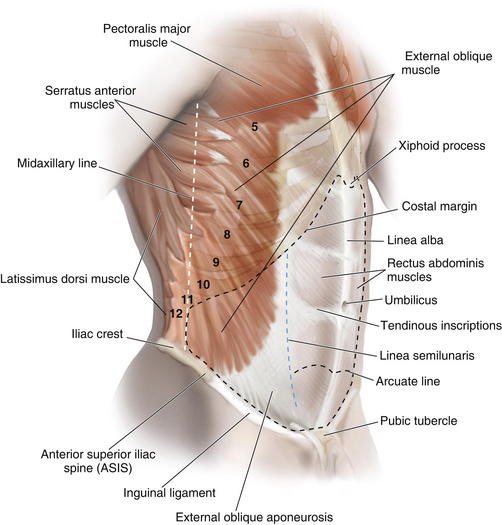
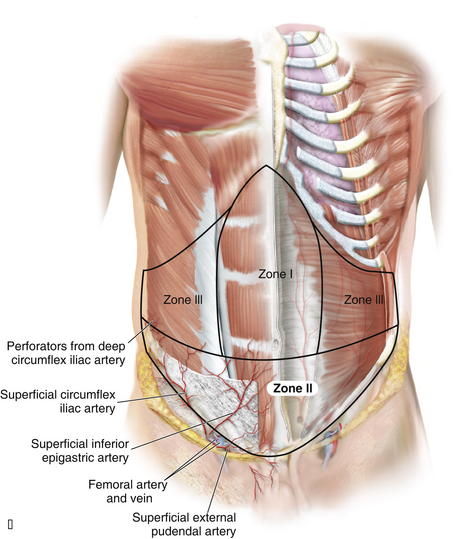
 The anterior abdominal wall (Figs. 1-1 to 1-3) is a hexagonal area defined superiorly by the costal margin and xiphoid process; laterally by the midaxillary line; and inferiorly by the symphysis pubis, pubic tubercle, inguinal ligament, anterior superior iliac spine, and iliac crest.
The anterior abdominal wall (Figs. 1-1 to 1-3) is a hexagonal area defined superiorly by the costal margin and xiphoid process; laterally by the midaxillary line; and inferiorly by the symphysis pubis, pubic tubercle, inguinal ligament, anterior superior iliac spine, and iliac crest.
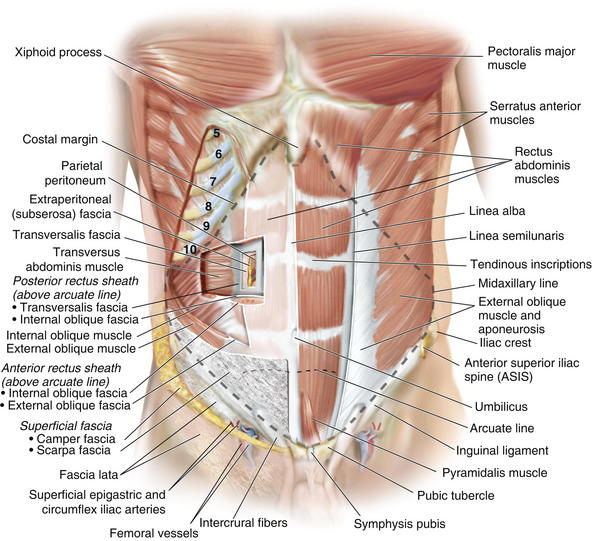
2 Superficial Fascial Layers (see Figs. 1-1 and 1-2)
 The superficial fascia of the abdominal wall consists of a single layer above the umbilicus, consisting of the fused Camper and Scarpa fasciae.
The superficial fascia of the abdominal wall consists of a single layer above the umbilicus, consisting of the fused Camper and Scarpa fasciae.



3 Deep Fascial Layers (see Figs. 1-1 and 1-2)


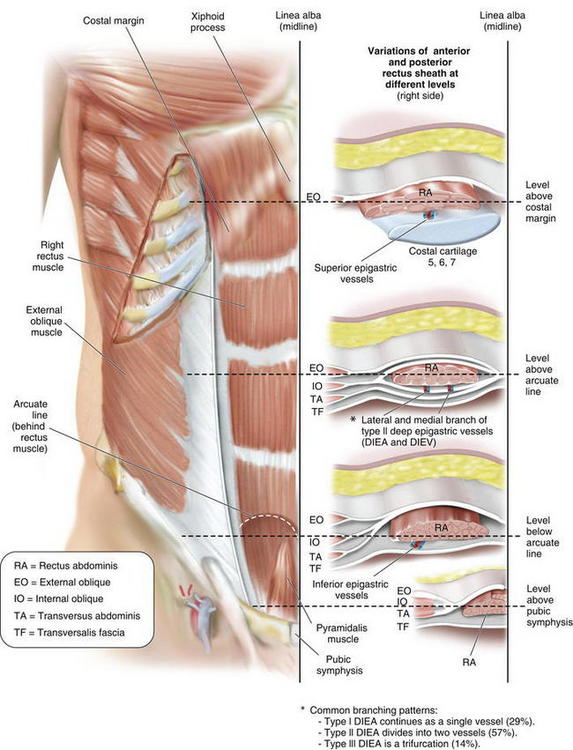
 The arcuate line (see Fig. 1-3) is located midway between the umbilicus and symphysis pubis and is a transition point where the posterior rectus sheath transitions from being the fusion of part of internal oblique fascia and transversalis fascia superiorly to only transversalis fascia inferiorly.
The arcuate line (see Fig. 1-3) is located midway between the umbilicus and symphysis pubis and is a transition point where the posterior rectus sheath transitions from being the fusion of part of internal oblique fascia and transversalis fascia superiorly to only transversalis fascia inferiorly.
 Below the arcuate line, the external oblique and internal oblique fasciae merge to form the anterior rectus sheath. The posterior rectus sheath consists of transversus abdominis fascia, making this only a thin layer with minimal strength.
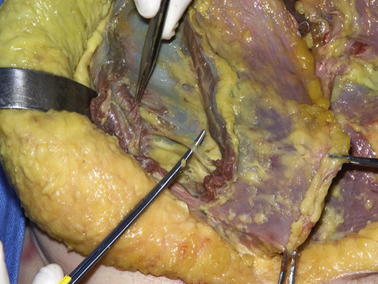
Below the arcuate line, the external oblique and internal oblique fasciae merge to form the anterior rectus sheath. The posterior rectus sheath consists of transversus abdominis fascia, making this only a thin layer with minimal strength. The linea alba results from fusion of the anterior and posterior rectus sheaths and lies in the midline, extending cranially from the xiphoid process to the pubic symphysis caudally Figure 1-4 shows the anterior wall fascia after dissection of the abdominal wall skin and subcutaneous tissue, showing the linea alba and linea semilunaris.
The linea alba results from fusion of the anterior and posterior rectus sheaths and lies in the midline, extending cranially from the xiphoid process to the pubic symphysis caudally Figure 1-4 shows the anterior wall fascia after dissection of the abdominal wall skin and subcutaneous tissue, showing the linea alba and linea semilunaris.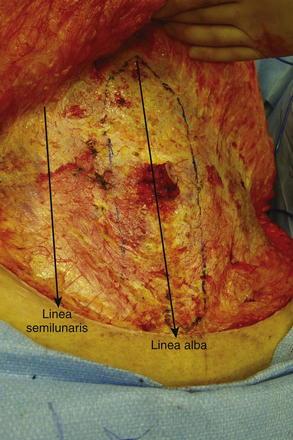
 Pearls and Pitfalls
Pearls and Pitfalls
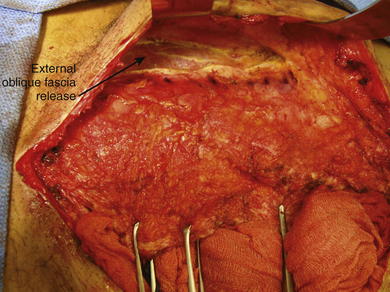
Incision, release, and dissection of the anterior external oblique fascia can be done for repair of ventral hernias. This technique is called the components separation (Fig. 1-5). The incision in the external oblique fascia is made 1 to 2 cm lateral to the linea semilunaris, and the fascia is released to attain primary closure. Incisions also can be made in the posterior rectus sheath to gain additional length.
4 Abdominal Wall Musculature (see Figs. 1-1 to 1-3)
 The paired rectus abdominis muscles are the principal flexors of the anterior abdominal wall. They function to stabilize the pelvis while walking. They also protect the abdominal organs and help in forced expiration.
The paired rectus abdominis muscles are the principal flexors of the anterior abdominal wall. They function to stabilize the pelvis while walking. They also protect the abdominal organs and help in forced expiration. The rectus abdominis muscles originate from the pubic symphysis and pubic crest and insert on the anterior surfaces of the fifth, sixth, and seventh costal cartilages and the xiphoid processes. Laterally, the rectus sheath merges with the aponeurosis of the external oblique muscles to form the linea semilunaris (Fig. 1-4).
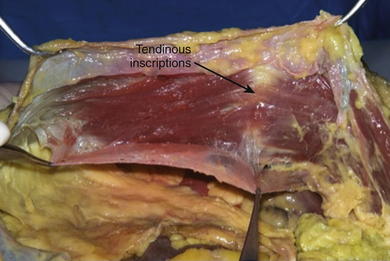
The rectus abdominis muscles originate from the pubic symphysis and pubic crest and insert on the anterior surfaces of the fifth, sixth, and seventh costal cartilages and the xiphoid processes. Laterally, the rectus sheath merges with the aponeurosis of the external oblique muscles to form the linea semilunaris (Fig. 1-4). Three to four tendinous inscriptions, which are adherent to the anterior rectus sheath, interrupt the rectus abdominis along its length (Fig. 1-6).
Three to four tendinous inscriptions, which are adherent to the anterior rectus sheath, interrupt the rectus abdominis along its length (Fig. 1-6).

 The transversus abdominis muscle is the deepest of the three lateral abdominal wall muscles and courses in a horizontal direction. It originates from the anterior three fourths of the iliac crest; lateral third of the inguinal ligament; and inner surface of the lower six costal cartilages, interdigitating with fibers of the diaphragm. The muscle ends medially in a broad flat aponeurosis, merging above the arcuate line with the posterior lamella of the internal oblique aponeurosis and the linea alba. Below the arcuate line, it inserts into the pubic crest and pectineal line, forming the conjoint tendon with the internal oblique.
The transversus abdominis muscle is the deepest of the three lateral abdominal wall muscles and courses in a horizontal direction. It originates from the anterior three fourths of the iliac crest; lateral third of the inguinal ligament; and inner surface of the lower six costal cartilages, interdigitating with fibers of the diaphragm. The muscle ends medially in a broad flat aponeurosis, merging above the arcuate line with the posterior lamella of the internal oblique aponeurosis and the linea alba. Below the arcuate line, it inserts into the pubic crest and pectineal line, forming the conjoint tendon with the internal oblique.


5 Neurovascular Supply of the Abdominal Wall
 Pearls and Pitfalls
Pearls and Pitfalls

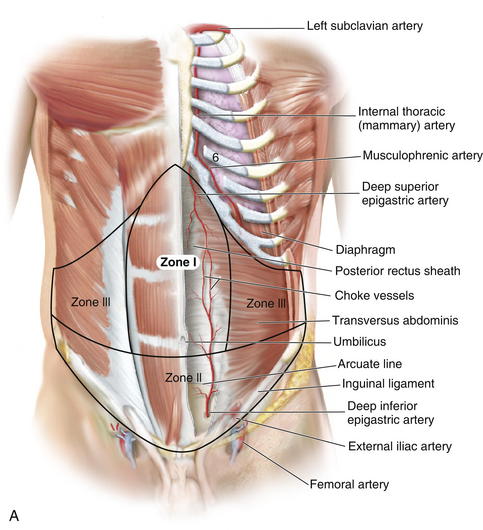
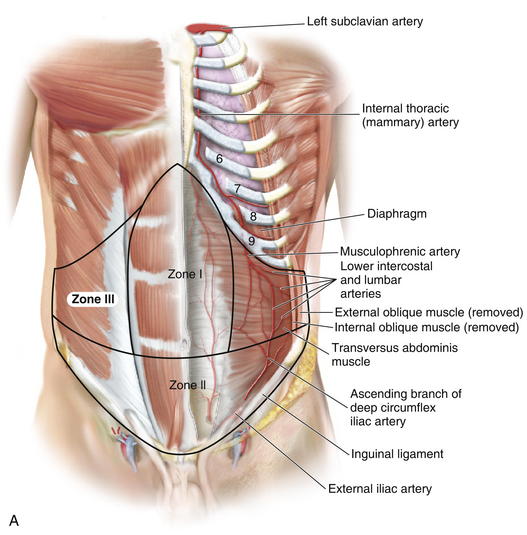
 Zone I consists of the upper and midcentral abdominal walls and is supplied by the vertically oriented deep superior (Fig. 1-7, A).and deep inferior epigastric arteries (Fig. 1-7, B).
Zone I consists of the upper and midcentral abdominal walls and is supplied by the vertically oriented deep superior (Fig. 1-7, A).and deep inferior epigastric arteries (Fig. 1-7, B). Zone II consists of the lower abdominal wall and is supplied by the epigastric arcade, superficial inferior epigastric, superficial external pudendal, and superficial circumflex iliac arteries. Perforators from the deep circumflex iliac arteries also supply a region of skin posterior and cephalad to the anterior superior iliac spine along the axis of the iliac crest.
Zone II consists of the lower abdominal wall and is supplied by the epigastric arcade, superficial inferior epigastric, superficial external pudendal, and superficial circumflex iliac arteries. Perforators from the deep circumflex iliac arteries also supply a region of skin posterior and cephalad to the anterior superior iliac spine along the axis of the iliac crest.
 Vascular Supply
Vascular Supply
 Knowledge of these zones of blood supply to the anterior abdominal wall is important when planning incisions for surgical procedures. A previous subcostal incision can compromise the circulation to Huger’s zone III of the abdominal wall. In transverse rectus abdominis myocutaneous (TRAM) flap harvest, the presence of a subcostal scar was found to increase donor site complications, with a significantly higher incidence of abdominal wall skin necrosis (25%) compared with patients without abdominal wall scars (5%).
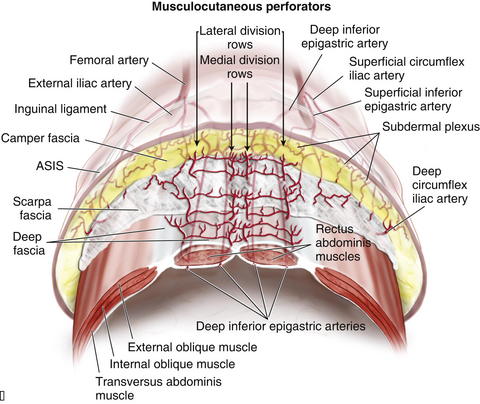
Knowledge of these zones of blood supply to the anterior abdominal wall is important when planning incisions for surgical procedures. A previous subcostal incision can compromise the circulation to Huger’s zone III of the abdominal wall. In transverse rectus abdominis myocutaneous (TRAM) flap harvest, the presence of a subcostal scar was found to increase donor site complications, with a significantly higher incidence of abdominal wall skin necrosis (25%) compared with patients without abdominal wall scars (5%). The superior epigastric artery and deep inferior epigastric arteries lie on the posterior aspect of the rectus abdominis muscles and supply the muscle and overlying skin and subcutaneous tissue through musculocutaneous perforators (Fig. 1-9).
The superior epigastric artery and deep inferior epigastric arteries lie on the posterior aspect of the rectus abdominis muscles and supply the muscle and overlying skin and subcutaneous tissue through musculocutaneous perforators (Fig. 1-9). A study by Saber et al. (2004) provides guidelines for location of the epigastric vessels based on computed tomography (CT) scan data in 100 patients. At the xiphoid process, the superior epigastric arteries (SEA) were 4.41 ± 0.13 cm from the midline on the right and 4.53 ± 0.14 cm from the left. Midway between xiphoid and umbilicus, the SEA was 5.50 ± 0.16 cm on right of midline and 5.36 ± 0.16 cm on the left. At the umbilicus, the epigastric vessels were 5.88 ± 0.14 cm on the right and 5.55 ± 0.13 on left of midline. Midway between umbilicus and symphysis pubis, the inferior epigastric arteries (IEA) were 5.32 ± 0.12 cm on right and 5.25 ± 0.11 cm on left of midline. While at the symphysis pubis, the IEA were 7.47 ± 0.10 cm from the midline on the right and 7.49 ± 0.09 cm from midline on the left side.
A study by Saber et al. (2004) provides guidelines for location of the epigastric vessels based on computed tomography (CT) scan data in 100 patients. At the xiphoid process, the superior epigastric arteries (SEA) were 4.41 ± 0.13 cm from the midline on the right and 4.53 ± 0.14 cm from the left. Midway between xiphoid and umbilicus, the SEA was 5.50 ± 0.16 cm on right of midline and 5.36 ± 0.16 cm on the left. At the umbilicus, the epigastric vessels were 5.88 ± 0.14 cm on the right and 5.55 ± 0.13 on left of midline. Midway between umbilicus and symphysis pubis, the inferior epigastric arteries (IEA) were 5.32 ± 0.12 cm on right and 5.25 ± 0.11 cm on left of midline. While at the symphysis pubis, the IEA were 7.47 ± 0.10 cm from the midline on the right and 7.49 ± 0.09 cm from midline on the left side.


 The superior epigastric artery, when described, refers in general to the deep superior epigastric artery. A superficial superior epigastric artery has been noted in anatomic studies, but it is not clinically significant.
The superior epigastric artery, when described, refers in general to the deep superior epigastric artery. A superficial superior epigastric artery has been noted in anatomic studies, but it is not clinically significant.




 A study by Chowdhry et al. (2010) reported that the DIEA encountered the lateral border of the rectus abdominis at a mean distance of 10.45 ± 1.58 cm from the umbilicus, with the first perforator transversing the rectus abdominis muscle around 7.4 ± 1.64 cm from the umbilicus.
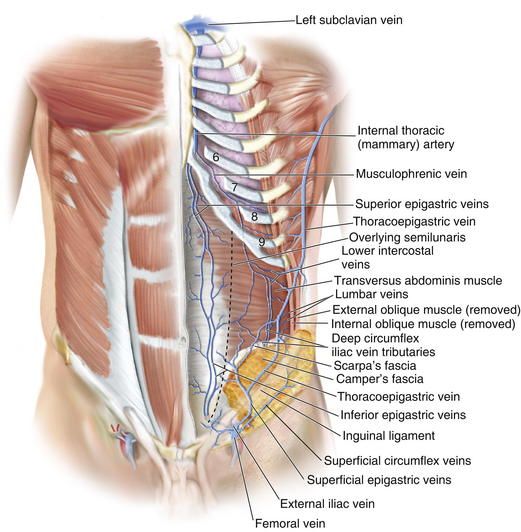
A study by Chowdhry et al. (2010) reported that the DIEA encountered the lateral border of the rectus abdominis at a mean distance of 10.45 ± 1.58 cm from the umbilicus, with the first perforator transversing the rectus abdominis muscle around 7.4 ± 1.64 cm from the umbilicus. Veins draining the anterior abdominal wall (Fig. 1-10) run as venae comitantes, accompanying the perforators and subsequently main arteries of the deep inferior and superior epigastric arteries. These ultimately drain into the azygos system and external iliac veins.
Veins draining the anterior abdominal wall (Fig. 1-10) run as venae comitantes, accompanying the perforators and subsequently main arteries of the deep inferior and superior epigastric arteries. These ultimately drain into the azygos system and external iliac veins.




 Nerve Supply (Fig. 1-11)
Nerve Supply (Fig. 1-11)
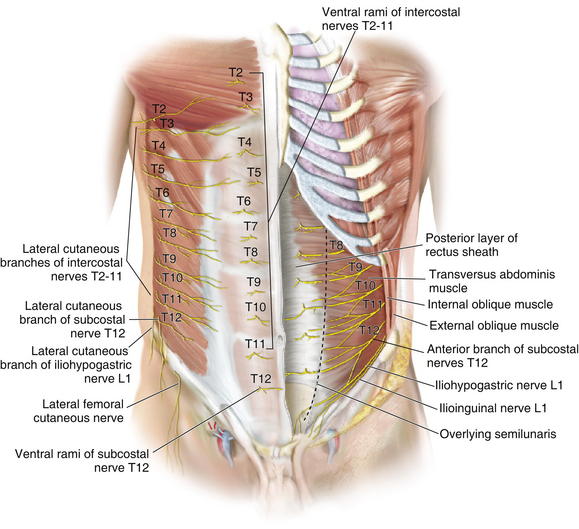
 Sensory innervation of the abdominal wall is derived from the anterior branches of the intercostals and subcostal nerves, from T7 to L1. These nerves run together with the intercostal and lumbar arteries in the plane between the internal oblique and transversalis muscles. Figure 1-12 shows the motor nerves to the rectus abdominis muscle. The internal oblique muscle has been divided, showing the nerve deep to the internal oblique muscle and superficial to the transversus abdominis muscle.
Sensory innervation of the abdominal wall is derived from the anterior branches of the intercostals and subcostal nerves, from T7 to L1. These nerves run together with the intercostal and lumbar arteries in the plane between the internal oblique and transversalis muscles. Figure 1-12 shows the motor nerves to the rectus abdominis muscle. The internal oblique muscle has been divided, showing the nerve deep to the internal oblique muscle and superficial to the transversus abdominis muscle.









2 Abdominal Wall Physiology
1 Function in Respiration
 The abdominal wall plays an accessory role to the intercostal muscles, thorax, and diaphragm in respiration.
The abdominal wall plays an accessory role to the intercostal muscles, thorax, and diaphragm in respiration.











3 Abdominal Wall Disruption Relevant to Anatomy
1 Rectus Diastasis
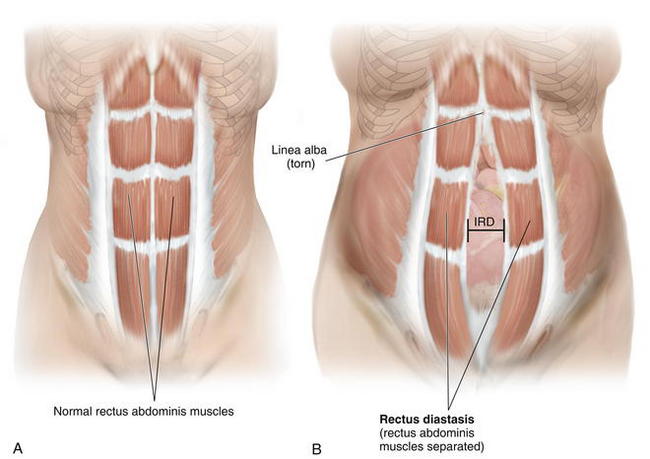
 Diastasis of the rectus abdominis muscles is defined as separation of the paired recti at the midline (Fig. 1-13).
Diastasis of the rectus abdominis muscles is defined as separation of the paired recti at the midline (Fig. 1-13).





2 Ventral Hernia
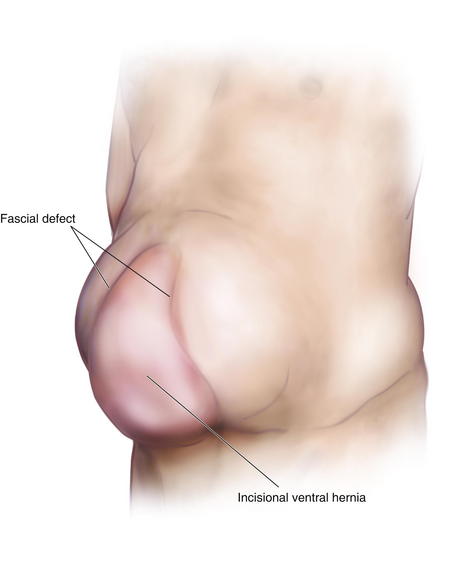
 Ventral hernia typically develops as an incisional hernia, following a midline laparotomy through the linea alba; it is due to incomplete healing that results in a fascial defect.
Ventral hernia typically develops as an incisional hernia, following a midline laparotomy through the linea alba; it is due to incomplete healing that results in a fascial defect.





3 Physiology of Ventral Hernia Formation









Atisha D., Alderman A.K. A systematic review of abdominal wall function following abdominal flaps for post mastectomy breast reconstruction. Ann Plast Surg. 2009;63:222-230.
Blanchard P.D. Diastasis recti abdominis in HIV-infected men with lipodystrophy. HIV Med. 2005;6:54-56.
Boyd J.B., Taylor G.I., Corlett R. The vascular territories of the superior epigastric and the deep inferior epigastric systems. Plast Reconstr Surg. 1984;73:1-16.
Chowdhry S., Hazani R., Collis P., Wilhelmi B.J. Anatomical landmarks for safe elevation of the deep inferior epigastric perforator flap: a cadaveric study. Eplasty. 2010;10:e41.
DuBay D.A., Choi W., Urbanchek M.G., et al. Incisional herniation induces decreased abdominal wall compliance via oblique muscle atrophy and fibrosis. Ann Surg. 2007;245:140-146.
Ducic I., Moxley M., Al-Attar A. Algorithm for treatment of postoperative incisional groin pain after cesarean delivery or hysterectomy. Obstet Gynecol. 2006;108:27-31.
El-Mrakby H.H., Milner R.H. The vascular anatomy of the lower anterior abdominal wall: a microdissection study on the deep inferior epigastric vessels and the perforator branches. Plast Reconstr Surg. 2002;109:539-543.
Franz M.G. The biology of hernia formation. Surg Clin North Am. 2008;88:1-15.
Hartrampf C.R., Scheflan M., Black P.W. Breast reconstruction with a transverse abdominal island flap. Plast Reconstr Surg. 1982;69:216-225.
Hsia M., Jones S. Natural resolution of rectus abdominis diastasis. Two single case studies. Aust J Physiother. 2000;46:301-307.
Huger W.E.Jr. The anatomic rationale for abdominal lipectomy. Am Surg. 1979;45:612-617.
Losken A., Carlson G.W., Jones G.E., Culbertson J.H., Schoemann M., Bostwick J.3rd. Importance of right subcostal incisions in patients undergoing TRAM flap breast reconstruction. Ann Plast Surg. 2002;49:115-119.
Moesbergen T., Law A., Roake J., Lewis D.R. Diastasis recti and abdominal aortic aneurysm. Vascular. 2009;17:325-329.
Moon H.K., Taylor G.I. The vascular anatomy of rectus abdominis musculocutaneous flaps based on the deep superior epigastric system. Plast Reconstr Surg. 1988;82:815-832.
Ramirez O.M., Ruas E., Dellon A.L. “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg. 1990;86:519-526.
Rozen W.M., Chubb D., Grinsell D., Ashton M.W. The variability of the superficial inferior epigastric artery (SIEA) and its angiosome: A clinical anatomical study. Microsurgery. 2010 Jan 7. [Epub ahead of print]
Saber A.A., Meslemani A.M., Davis R., Pimental R. Safety zones for anterior abdominal wall entry during laparoscopy: a CT scan mapping of epigastric vessels. Ann Surg. 2004;239:182-185.
Schneid H., Vazquez M.P., Vacher C., Gormelen M., Cabrol S., Le Bouc Y. The Beckwith-Wiedemann syndrome phenotype and the risk of cancer. Med Pediatr Oncol. 1997;28:411-415.
Taylor G.I. The angiosomes of the body and their supply to perforator flaps. Clin Plast Surg. 2003;30:331-342.
Wong C., Saint-Cyr M., Mojallal A., et al. Perforasomes of the DIEP flap: vascular anatomy of the lateral versus medial row perforators and clinical implications. Plast Reconstr Surg. 2010;125:772-782.
