Chapter 5 Abdominal Pain
1 Why is the evaluation of abdominal pain especially challenging in the pediatric patient?
Pollack ES: Pediatric abdominal surgical emergencies. Pediatr Ann 25:448–457, 1996.
2 How can I organize my approach to the patient?
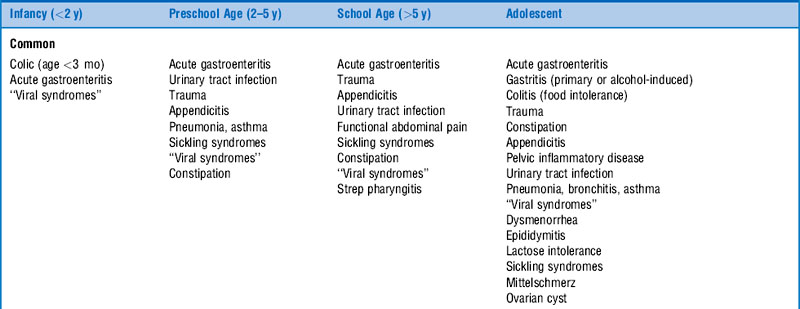
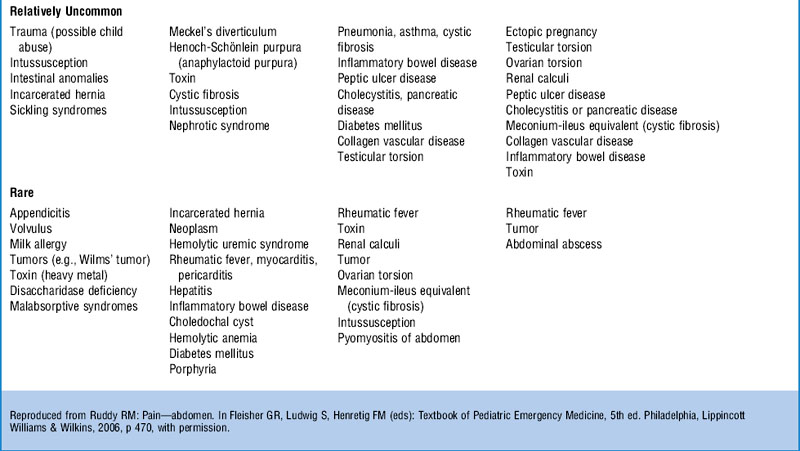
In the unstable patient, the initial approach should begin with an assessment of the patient’s airway, breathing, and circulation. Following stabilization, obtain a complete history and perform a physical examination. The history and physical examination are the essential components of the evaluation. Elicit the nature of the pain, such as its onset, quality, location, and duration, as well as the presence of any associated symptoms. The differential diagnosis of abdominal pain in children is extensive (Table 5-1). The age of the patient and the most likely diagnoses in that age group can be used in concert with the history and physical examination to narrow the differential and guide further diagnostic testing.












5 How can I maximize the physical examination of the pediatric patient with abdominal pain?
6 Does the use of IV analgesia affect the diagnostic accuracy of the physical examination in children with significant abdominal pain of unknown etiology?
9 What are the two most common causes of acute abdominal emergencies in children?
Appendicitis is the most common cause in the United States, followed by intussusception.
Pollack ES: Pediatric abdominal surgical emergencies. Pediatr Ann 25:448–457, 1996.
10 What is the typical presentation of appendicitis in children?
D’Agostino J: Common abdominal emergencies in children. Pediatric Emerg Med 20:139–153, 2002.
12 Discuss the test characteristics (e.g., sensitivity, specificity) of limited computed tomography (CT) with rectal contrast in the evaluation of children with suspected appendicitis.
15 In which patients should the diagnosis of intussusception be considered?
Klein EJ, Kapoor D, Shugerman RP: The diagnosis of intussusception. Clin Pediatr 43:343–347, 2004.



