Abdominal Enterocele Repair
Weakness in the support of the cervix or the vaginal vault can lead to uterovaginal prolapse or posthysterectomy vault prolapse. These defects are usually associated with an enterocele, a defect that results in attenuation or breakage of the rectovaginal or pubocervical fascia and thus allows the peritoneum to come into direct contact with the vaginal epithelium.
The posterior cul-de-sac (Fig. 41–1) should be addressed routinely when abdominal hysterectomy is performed, as well as in selected cases of retropubic urethropexy. At the time of abdominal hysterectomy, it is important to reconnect the vaginal vault to the cardinal uterosacral ligament complex (Fig. 41–2). Also, the continuity of the pelvic floor must be reinstated by approximating the fascia of the anterior vaginal wall (Figs. 41–3 and 41–4) to the fascia of the posterior vaginal wall (Fig. 41–5).
Three techniques of abdominal enterocele repair have been described: the Moschcowitz and Halban procedures and uterosacral ligament plication. The Moschcowitz procedure is performed by placing concentric purse string sutures around the cul-de-sac to include the posterior vaginal wall, the right pelvic sidewall, the serosa of the sigmoid, and the left pelvic sidewall (Figs. 41–6 and 41–7). The initial suture is placed at the base of the cul-de-sac. Usually three or four sutures completely obliterate the cul-de-sac. The purse string sutures are tied so that no small defects remain that could entrap small bowel or lead to enterocele recurrence. Care should be taken not to include the ureter in the purse string sutures or to allow the ureter to be kinked medially when the sutures are tied.
Halban described his technique to obliterate the cul-de-sac by using sutures placed sagittally between the uterosacral ligaments. Four or five sutures are placed in a longitudinal fashion sequentially through the serosa of the sigmoid, into the deep peritoneum of the cul-de-sac, and up the posterior vaginal wall (Figs. 41–8 through 41–10). The sutures are tied, obliterating the cul-de-sac (Fig. 41–11).
Transverse plication of the uterosacral ligaments can be used also to obliterate the cul-de-sac (Fig. 41–12). Three to five sutures are placed into the medial portion of the uterosacral ligament, through the back of the vagina, and through the opposite uterosacral ligament. The lowest sutures incorporate the anterior rectal serosa to bring the rectum adjacent to the uterosacral ligaments and vagina (Figs. 41–13 and 41–14). Care must be taken to avoid injury or kinking of the ureter. Relaxing incisions can be made in the peritoneum lateral to the uterosacral ligaments to release the ureter if necessary.
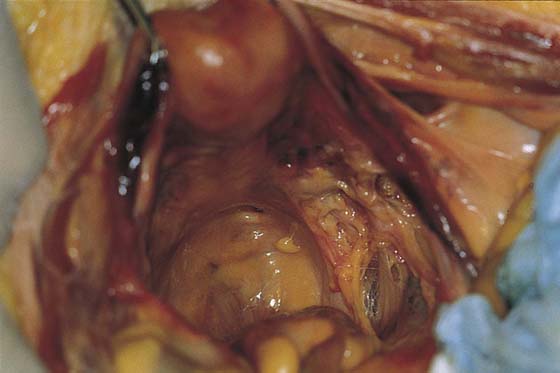
FIGURE 41–1 Prominent cul-de-sac noted with uterus in place.
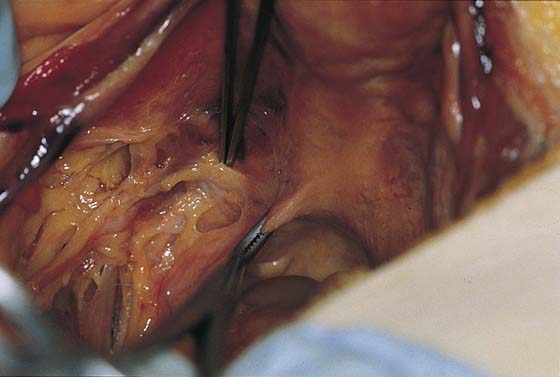
FIGURE 41–2 Left uterosacral (clamped) and left cardinal ligaments. These structures are responsible for support of the cervix and the upper vagina.
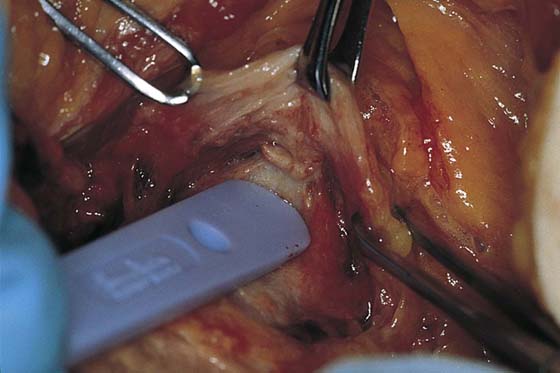
FIGURE 41–3 The pubocervical fascia has been sharply dissected off the anterior cervix and vagina at the time of abdominal hysterectomy.
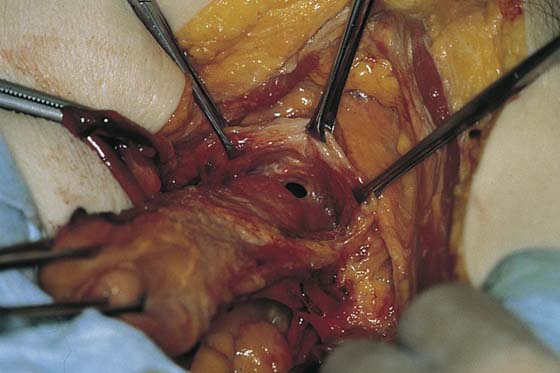
FIGURE 41–4 The pubocervical fascia has been mobilized below the cervix. The anterior vaginal wall has been penetrated in preparation for removal of the uterus.

FIGURE 41–5 The open vaginal cuff after removal of the uterus. Note the Allis clamps on the vaginal epithelium with the pubocervical fascia anteriorly and the vaginal epithelium with that rectovaginal fascia posteriorly. Closure of the cuff thus will restore fascial continuity between the anterior and posterior vaginal walls.
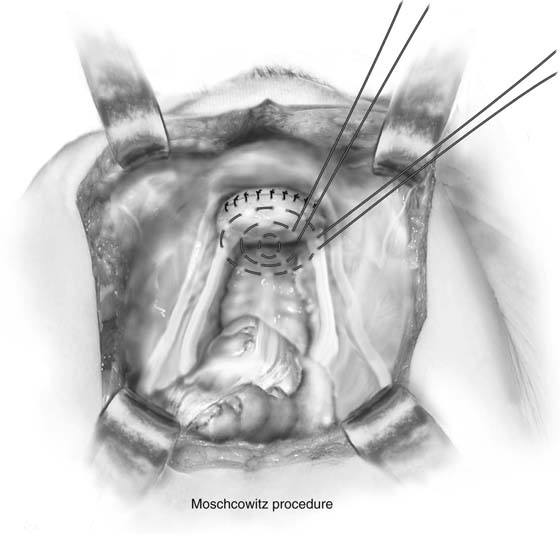
FIGURE 41–6 Moschcowitz procedure. Concentric purse string sutures are placed in the cul-de-sac. The suture should include the back of the vagina, the sidewall of the pelvis at the level of the distal uterosacral ligament, and the serosa of the sigmoid colon.

FIGURE 41–7 Moschcowitz closure of the cul-de-sac. Initial purse string suture has been placed.
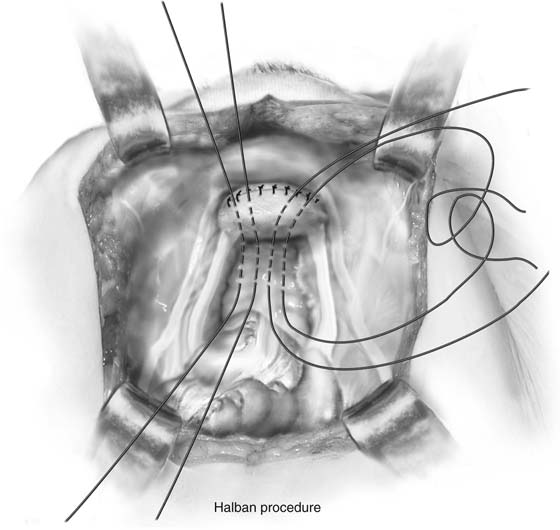
FIGURE 41–8 Halban closure of the cul-de-sac. Sutures are placed longitudinally through the serosa of the sigmoid, into the deep peritoneum of the cul-de-sac, and up the posterior vaginal wall.

FIGURE 41–9 Halban closure of the cul-de-sac showing suture placement. Clamps are placed on the vaginal vault for traction.
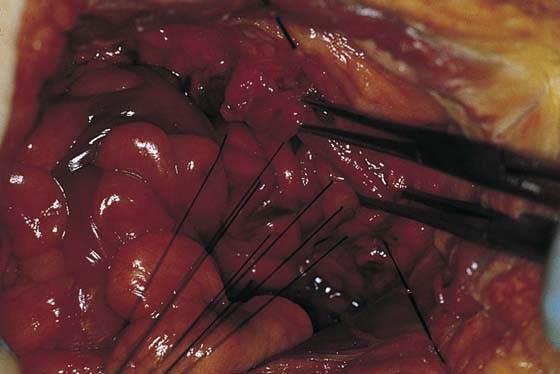
FIGURE 41–10 Halban closure of the cul-de-sac. Pulling up of sutures brings the sigmoid into contact with the posterior vaginal wall.
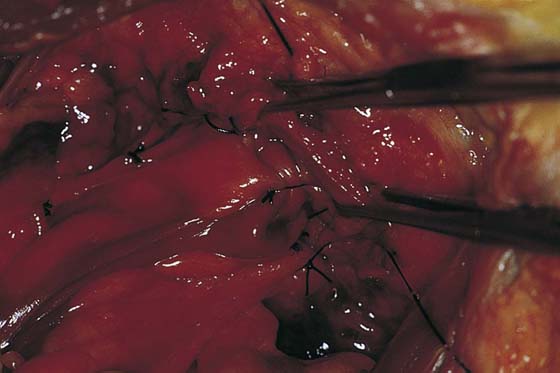
FIGURE 41–11 Halban closure of the cul-de-sac. Tying of the sutures completely obliterates the cul-de-sac.
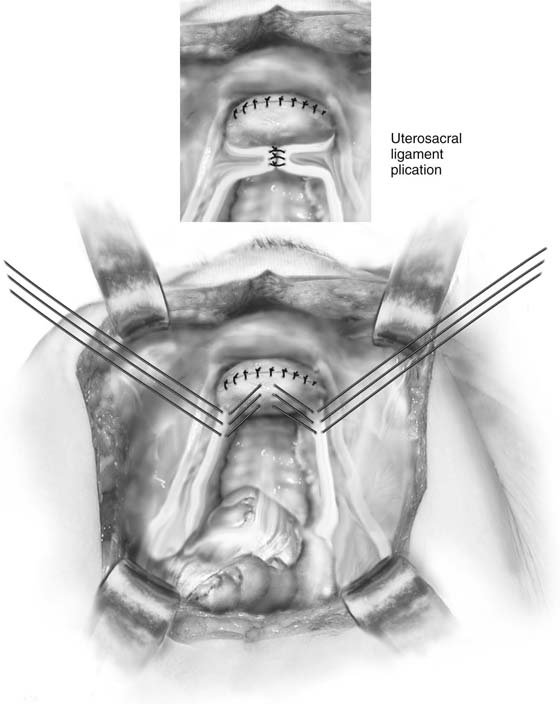
FIGURE 41–12 Abdominal plication of the uterosacral ligament.

FIGURE 41–13 A series of sutures have been placed to incorporate the uterosacral ligaments across the midline.
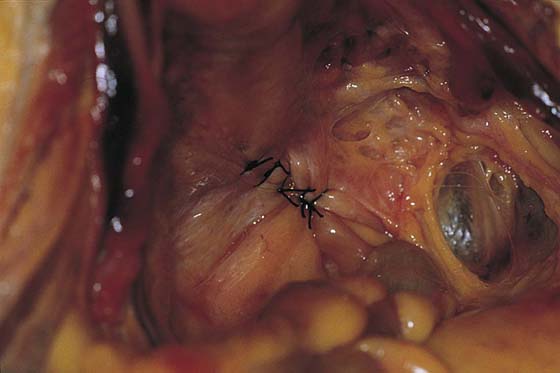
FIGURE 41–14 Sutures have been cut. Note that the uterosacral ligaments have been plicated across midline, completely obliterating the cul-de-sac.






