Tubo-Ovarian Abcess and Pelvic Inflammatory Disease
Synonyms/Description
Etiology
Ultrasound Findings
Differential Diagnosis
Clinical Aspects and Recommendations
Figures
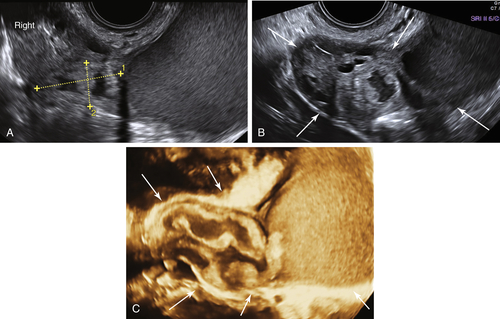
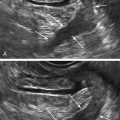
Figure T5-1 Very large pyosalpinx in a very sick patient with severe PID. A and B show the 2-D view of the very large pyosalpinx. The distal end of the tube is filled with a large amount of echogenic fluid. The rest of tube is more narrow and folded upon itself (calipers and arrows). C is a 3-D rendering of the entire dilated tube (arrows).
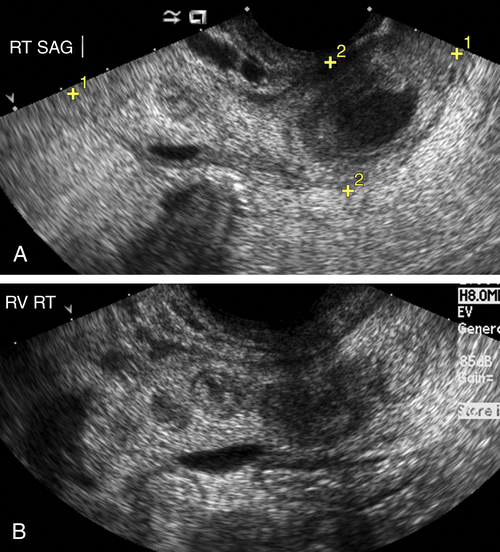
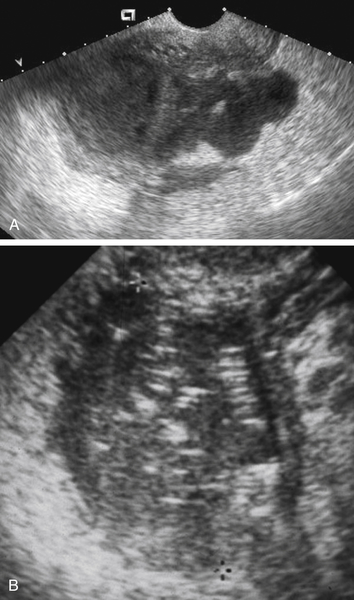
Figure T5-3 Tubo-ovarian abscess in two different patients. A shows a large complex cystic mass with irregular borders and septations in a patient with severe PID. Note that the borders of the mass are indistinct and blurry because of the surrounding edema. Although the sonographic appearance of the mass is nonspecific, the setting of a septic patient helps to make the diagnosis more definitive. B shows a completely solid adnexal mass containing small linear echoes throughout, consistent with an air-containing abscess.
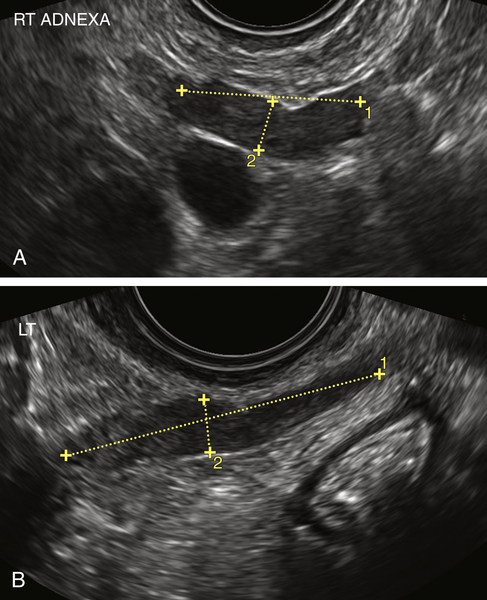
Figure T5-4 A and B, Salpingitis in two different patients. Note the elongated and straight swollen-appearing tubes (calipers). Both patients had localized pain in the area of the tube. For the patient in A, the diagnosis of pyosalpinx was confirmed at laparoscopy. The second patient improved with antibiotics.
Suggested Reading
Chappell C.A., Wiesenfeld H.C. Pathogenesis, diagnosis, and management of severe pelvic inflammatory disease and tuboovarian abscess. Clin Obstet Gynecol. 2012;55:893–903.
Cicchiello L.A., Hamper U.M., Scoutt L.M. Ultrasound evaluation of gynecologic causes of pelvic pain. Obstet Gynecol Clin North Am.. 2011;38:85–114.
Crossman S.H. The challenge of pelvic inflammatory disease. Am Fam Physician. 2006;73:859–864.
Ghiatas A.A. The spectrum of pelvic inflammatory disease. Eur Radiol. 2004;14(suppl):E184–E192.
Kamaya A., Shin L., Chen B., Desser T.S. Emergency gynecologic imaging. Semin Ultrasound CT MRI. 2008;29:353–368.
Kim M.Y., Rha S.E., Oh S.N., Jung S.E., Lee Y.J., Kim Y.S., Byun J.Y., Lee A., Kim M.R. MR imaging findings of hydrosalpinx: a comprehensive review. Radiographics. 2009;29:495–507.
Soper D.E. Pelvic inflammatory disease. Obstet Gynecol. 2010;116:419–428.
Varras M., Polyzos D., Perouli E., Noti P., Pantazis I., Akrivis C.H. Tubo-ovarian abscesses: spectrum of sonographic findings with surgical and pathological correlations. Clin Exp Obstet Gynecol. 2003;30:117–121.