[level-membership-for-surgery-category]
Problem 37 A 47-year-old man with lethargy and hypertension
A 47-year-old car salesman attends the emergency department with a spontaneous epistaxis. His nose is packed before undergoing cautery by the ENT surgeons. He remarks that he has not been feeling particularly well over the last few weeks. He feels he is somewhat lacking in energy which he had attributed to not eating due to a lack of appetite. This has led to him having to bring his belt in by two notches. On questioning he admits to more frequent headaches than usual. He has not experienced any dysuria or symptoms of prostatism. He has had no vomiting or diarrhoea. He has not had any abdominal pain.
He has never attended the hospital before and thinks the last time he saw his general practitioner was as a child for a sore throat. He takes no regular medication apart from paracetamol for his headaches. His alcohol consumption averages around 30 units per week. He smoked 20 cigarettes per day until 6 years ago.
Examination reveals a rather unwell-looking gentleman. He is apyrexial, and neither cyanosed, jaundiced nor clinically anaemic. His heart rate is 68 beats per minute in sinus rhythm and his heart sounds are normal. Blood pressure is markedly elevated at 214/112 mmHg. His jugular venous pulse is not visible. Auscultation of his chest reveals vesicular breath sounds throughout with no added sounds. Palpation of his abdomen reveals no masses nor are there any ascites. There are, however, some excoriations which the patient believes are due to a new detergent his wife is using. There is no ankle oedema. Fundoscopy shows grade two hypertensive retinopathy. Neurological examination yields no abnormality.
You decide to admit him for further investigation.
The following blood results become available.
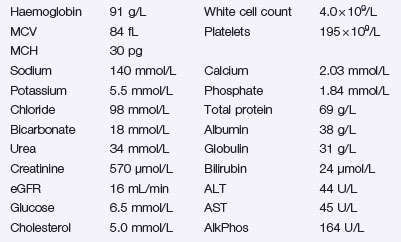
Answers
• Hypocalcaemia and hyperphosphataemia along with an elevated alkaline phosphatase are a consequence of the failure of hydroxylation of vitamin D and secondary hyperparathyroidism.
Other abnormalities include a mild metabolic acidosis and slightly elevated potassium.
A.5 The initial investigation of choice is renal ultrasound.
The pelvicaliceal system can be evaluated for the presence of hydronephrosis and renal stone disease
• Preventing or slowing further decline in renal function. This is achieved by maintaining tight blood pressure control and aggressive management of other co-morbidities like diabetes which may accelerate a fall in GFR. ACE inhibitors and angiotensin receptor blockers are effective in reducing proteinuria and slowing disease progression.
• Preparing for the possibility of needing renal replacement therapy. This begins with patient education, often with specialist nursing staff. Haemodialysis and peritoneal dialysis can be discussed with appropriate patients. Ideally dialysis access, i.e. arterio-venous fistulas, should be in place before the patient becomes dialysis dependent. Transplantation can be discussed. For some individuals the existence of a matched related donor may mean transplantation is a viable first-line option.
• Management of the distal consequences of renal failure. Renal anaemia will require correction with subcutaneous injections of erythropoietin. Some individuals require iron infusions. Renal bone disease will need to be addressed. Calcium and phosphate homeostasis will need to be achieved using a combination of diet, phosphate binders, hydroxylated derivatives of vitamin D, and attention to parathyroid hormone levels.
• Attending to cardiovascular risk. Patients with renal failure are at a high risk of athero-embolic events. Thus attention to additional cardiovascular risk factors such as hyperlipidaemia is vital. Again meticulous control of blood pressure and diabetes are essential.
• He will need to see a renal dietician. Advice will be required on balancing restricted protein, phosphate and potassium intake with achieving adequate nutrition.
• Education is key. A patient who is engaged in their care will fare much better in achieving a longer time to dialysis dependence and avoiding the complications of chronic renal failure.
Factors that may precipitate dialysis on an urgent basis include:
Revision Points
Issues to Consider
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Problem 37 A 47-year-old man with lethargy and hypertension
A 47-year-old car salesman attends the emergency department with a spontaneous epistaxis. His nose is packed before undergoing cautery by the ENT surgeons. He remarks that he has not been feeling particularly well over the last few weeks. He feels he is somewhat lacking in energy which he had attributed to not eating due to a lack of appetite. This has led to him having to bring his belt in by two notches. On questioning he admits to more frequent headaches than usual. He has not experienced any dysuria or symptoms of prostatism. He has had no vomiting or diarrhoea. He has not had any abdominal pain.
He has never attended the hospital before and thinks the last time he saw his general practitioner was as a child for a sore throat. He takes no regular medication apart from paracetamol for his headaches. His alcohol consumption averages around 30 units per week. He smoked 20 cigarettes per day until 6 years ago.
Examination reveals a rather unwell-looking gentleman. He is apyrexial, and neither cyanosed, jaundiced nor clinically anaemic. His heart rate is 68 beats per minute in sinus rhythm and his heart sounds are normal. Blood pressure is markedly elevated at 214/112 mmHg. His jugular venous pulse is not visible. Auscultation of his chest reveals vesicular breath sounds throughout with no added sounds. Palpation of his abdomen reveals no masses nor are there any ascites. There are, however, some excoriations which the patient believes are due to a new detergent his wife is using. There is no ankle oedema. Fundoscopy shows grade two hypertensive retinopathy. Neurological examination yields no abnormality.
You decide to admit him for further investigation.
