• Much higher percentage of fundic polyps than in earlier studies
Caused by increased use of PPI medications
• Syndromic polyps have high association with cancer risk in stomach and other organs
e.g., familial polyposis, Peutz-Jeghers syndrome
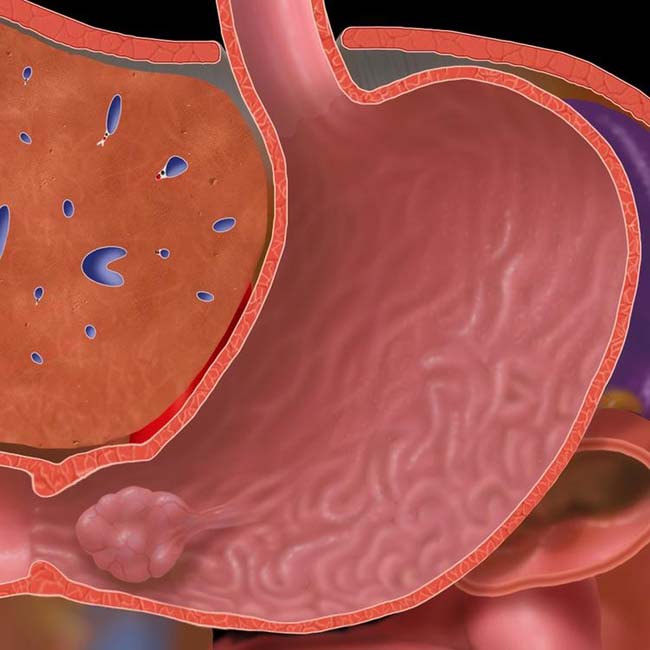
(Left) Graphic shows a pedunculated polyp in the gastric antrum, prone to prolapse through the pylorus with peristalsis. Any type of large polyp may prolapse in this fashion, including large hyperplastic, adenomatous, and even polypoid masses arising from the submucosa, such as lipomas.
(Right) Upper GI series shows a polypoid mass in the duodenal bulb that is a prolapsed gastric antral polyp (adenoma).
(Left) Film from an upper GI series in a 57-year-old man shows multiple small, sessile polyps in the gastric body. The appearance and age of the patient are typical for hyperplastic polyps.
(Right) Film from an upper GI series of adenomatous polyps in a patient with familial polyposis shows innumerable small polyps throughout the stomach. These are somewhat larger, more numerous, and more irregular in shape than most hyperplastic polyps.
TERMINOLOGY
Definitions
• Protruding, space-occupying lesion within stomach
Encompass a broad spectrum of conditions that may originate in gastric mucosa or submucosa
IMAGING
General Features
• Best diagnostic clue
Radiolucent filling defect, ring shadow, or contour defect on barium study
• Morphology
Hyperplastic polyps: Smooth, sessile
– Fundic gland polyps: Always sessile, multiple, small
Adenomatous polyps: Usually single with lobulated or cauliflower-like surface
Hamartomas: Cluster of broad-based polyps
• Other general features
Polyps classified based on pathology
Fundic gland polyps
– Variant of hyperplastic polyps (< 1 cm)
– Have become most common type of gastric polyp
– Associated with use of proton-pump inhibitor medication
Hyperplastic polyps
– Virtually no malignant potential
– Typical: Small, multiple, sessile (< 1 cm)
Location: Fundus and body
– Atypical large: Solitary, pedunculated (2-6 cm), location in body and antrum
– Atypical giant: Polyp (6-10 cm) multilobulated mass, location in body and antrum
Adenomatous polyps
– Less common (< 20% of benign polyps); dysplastic lesions
– Increased risk of malignant change via adenoma-carcinoma sequence
Much higher percentage of fundic polyps than in earlier studies
– FAP syndrome and PJS: 1 in 10,000 people
Natural History & Prognosis
• Complications
Risk of cancer in adenomatous polyp, FAP syndrome, and PJS
Gastric outlet obstruction
• Prognosis
Good: After removal of benign and cancer in situ polyp
Poor: Invasive carcinoma
Treatment
• Small (< 1 cm) and asymptomatic: Periodic surveillance
• Large (> 1 cm), sessile or pedunculated, and lobulated and symptomatic: Polypectomy
DIAGNOSTIC CHECKLIST
Consider
• Differentiate from other gastric discrete filling defects
• Check for family history of GI tract polyps
• Screen small intestine and colon to rule out associated hereditary polyposis syndromes
(Left) Film from an upper GI series in an elderly man with dysphagia shows a well-defined polyp at the GE junction.
(Right) Another spot film from the upper GI in the same patient shows the polyp prolapsing into the distal esophagus. Endoscopy and resection revealed an adenomatous gastric polyp.
(Left) Film from an upper GI series shows a well-defined polyp in the gastric body.
(Right) Endoscopic photograph in the same patient shows an ulcerated mass that was a benign adenoma. A band was placed around the base of the polyp, and it was resected at endoscopy.
(Left) Film from an upper GI series in an elderly man with dyspepsia shows a cluster of polypoid lesions arising from the gastric cardia and body. These have a smooth surface and most appear sessile.
(Right) Upper GI series in the same patient shows that some of the polyps appear to have a stalk . Endoscopy revealed multiple polyps with a villous adenoma histology.
Upper GI series shows a polypoid mass in the antrum that periodically prolapsed through the pylorus. This case proved to be leiomyoma.
Endoscopic photograph shows an antral polyp (adenoma) that intermittently prolapsed through the pylorus .
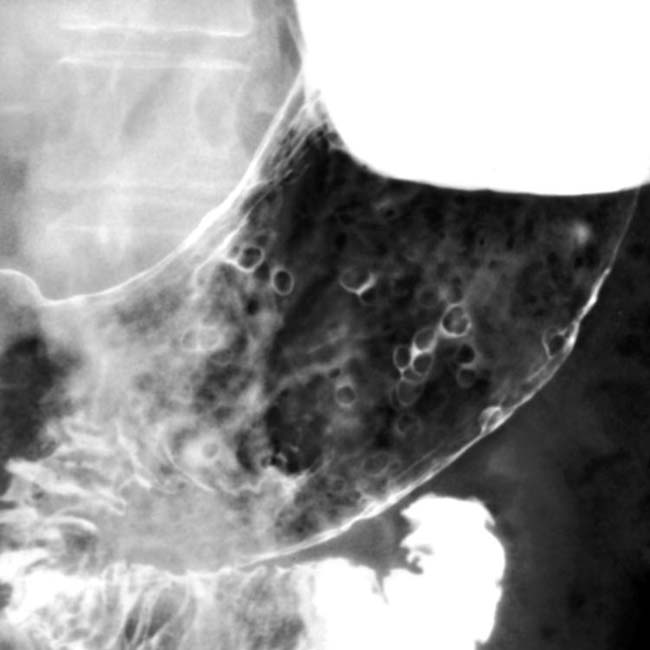
Upper GI series shows dozens of small hyperplastic gastric polyps.
Upper GI series shows multiple hyperplastic gastric polyps.
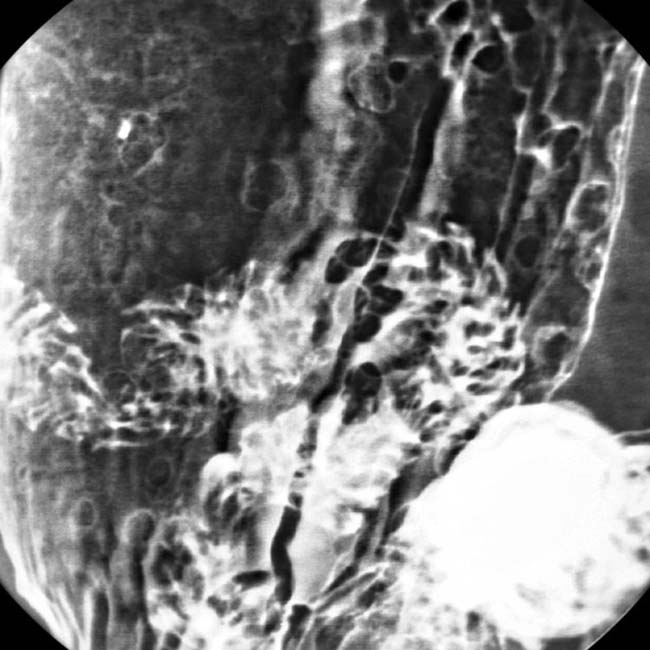
Upper GI series shows a large adenomatous gastric polyp .
Axial CECT shows a large gastric adenomatous polyp prolapsed into the duodenum.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Hyperplastic, adenomatous, and hamartomatous
• Fundic gland polyps: Now most common type
Associated with use of proton pump inhibitor (PPI) medication
Sometimes considered a variant of hyperplastic polyps
• Hyperplastic polyps
Virtually no malignant potential
Typical: Small, multiple, sessile (< 1 cm)
Location: Fundus and body
• Adenomatous polyps
Less common (< 20% of benign polyps)
Increased risk of malignant change
Usually solitary, > 1 cm
• Hamartomatous polyps
Peutz-Jeghers syndrome
Can occur as isolated finding (sporadic)
TOP DIFFERENTIAL DIAGNOSES
• Retained food and pills
• Gastric carcinoma (polypoid type)
• Gastric metastases and lymphoma
• Gastric gastrointestinal stromal tumor
• Ectopic pancreatic tissue
CLINICAL ISSUES
• Prevalence of gastric polyps in patients who have upper endoscopy = 6% (2009 study)
• Much higher percentage of fundic polyps than in earlier studies
Caused by increased use of PPI medications
• Syndromic polyps have high association with cancer risk in stomach and other organs
e.g., familial polyposis, Peutz-Jeghers syndrome
(Left) Graphic shows a pedunculated polyp in the gastric antrum, prone to prolapse through the pylorus with peristalsis. Any type of large polyp may prolapse in this fashion, including large hyperplastic, adenomatous, and even polypoid masses arising from the submucosa, such as lipomas.
(Right) Upper GI series shows a polypoid mass in the duodenal bulb that is a prolapsed gastric antral polyp (adenoma).
(Left) Film from an upper GI series in a 57-year-old man shows multiple small, sessile polyps in the gastric body. The appearance and age of the patient are typical for hyperplastic polyps.
(Right) Film from an upper GI series of adenomatous polyps in a patient with familial polyposis shows innumerable small polyps throughout the stomach. These are somewhat larger, more numerous, and more irregular in shape than most hyperplastic polyps.
TERMINOLOGY
Definitions
• Protruding, space-occupying lesion within stomach
Encompass a broad spectrum of conditions that may originate in gastric mucosa or submucosa
IMAGING
General Features
• Best diagnostic clue
Radiolucent filling defect, ring shadow, or contour defect on barium study
• Morphology
Hyperplastic polyps: Smooth, sessile
– Fundic gland polyps: Always sessile, multiple, small
Adenomatous polyps: Usually single with lobulated or cauliflower-like surface
Hamartomas: Cluster of broad-based polyps
• Other general features
Polyps classified based on pathology
Fundic gland polyps
– Variant of hyperplastic polyps (< 1 cm)
– Have become most common type of gastric polyp
– Associated with use of proton-pump inhibitor medication
Hyperplastic polyps
– Virtually no malignant potential
– Typical: Small, multiple, sessile (< 1 cm)
Location: Fundus and body
– Atypical large: Solitary, pedunculated (2-6 cm), location in body and antrum
– Atypical giant: Polyp (6-10 cm) multilobulated mass, location in body and antrum
Adenomatous polyps
– Less common (< 20% of benign polyps); dysplastic lesions
– Increased risk of malignant change via adenoma-carcinoma sequence













 in the duodenal bulb that is a prolapsed gastric antral polyp (adenoma).
in the duodenal bulb that is a prolapsed gastric antral polyp (adenoma).
 in the gastric body. The appearance and age of the patient are typical for hyperplastic polyps.
in the gastric body. The appearance and age of the patient are typical for hyperplastic polyps.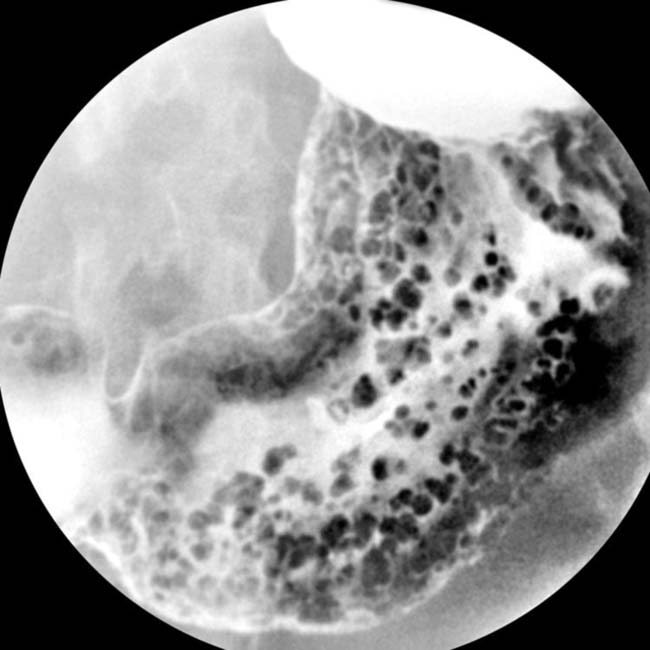





















































 at the GE junction.
at the GE junction.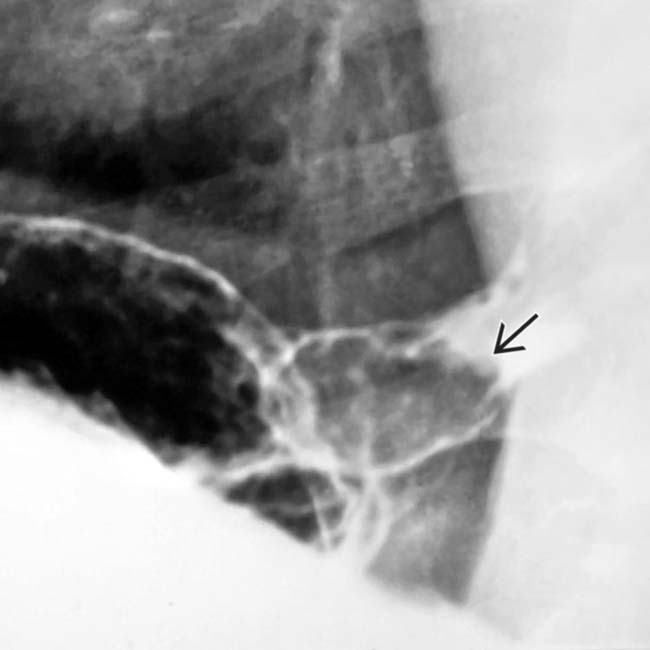
 prolapsing into the distal esophagus. Endoscopy and resection revealed an adenomatous gastric polyp.
prolapsing into the distal esophagus. Endoscopy and resection revealed an adenomatous gastric polyp.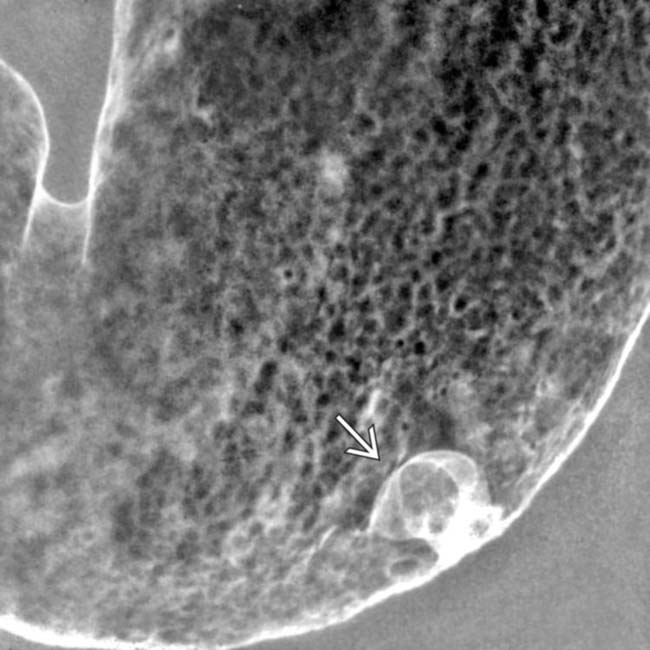
 in the gastric body.
in the gastric body.
 that was a benign adenoma. A band was placed around the base of the polyp, and it was resected at endoscopy.
that was a benign adenoma. A band was placed around the base of the polyp, and it was resected at endoscopy.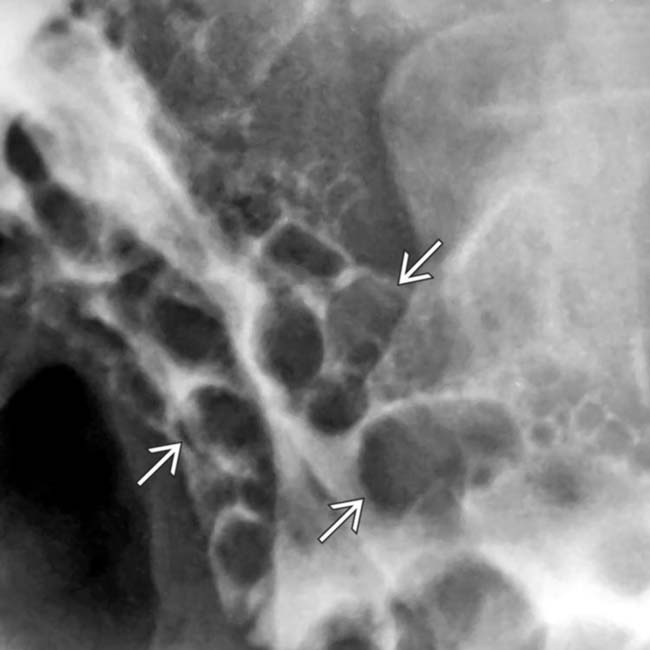
 arising from the gastric cardia and body. These have a smooth surface and most appear sessile.
arising from the gastric cardia and body. These have a smooth surface and most appear sessile.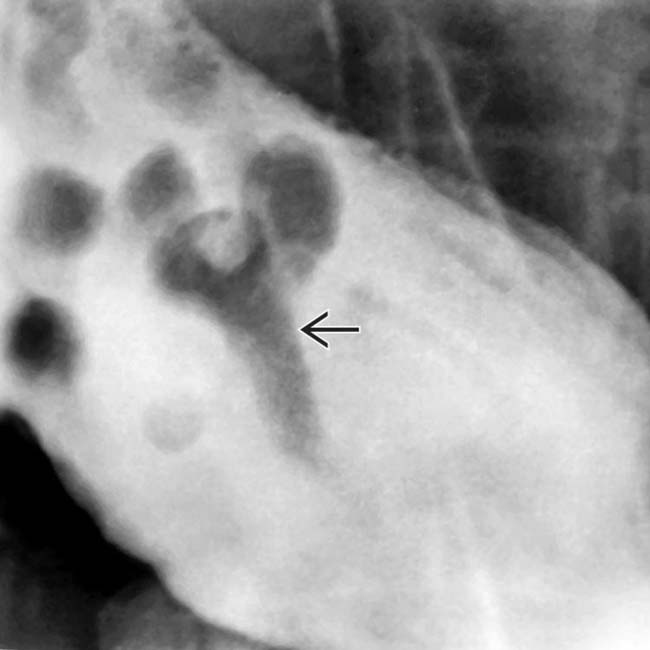
 . Endoscopy revealed multiple polyps with a villous adenoma histology.
. Endoscopy revealed multiple polyps with a villous adenoma histology.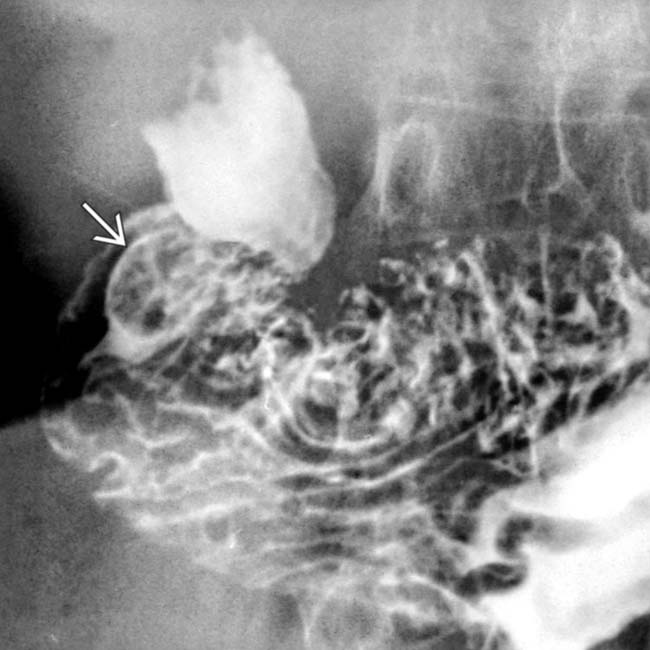
 in the antrum that periodically prolapsed through the pylorus. This case proved to be leiomyoma.
in the antrum that periodically prolapsed through the pylorus. This case proved to be leiomyoma.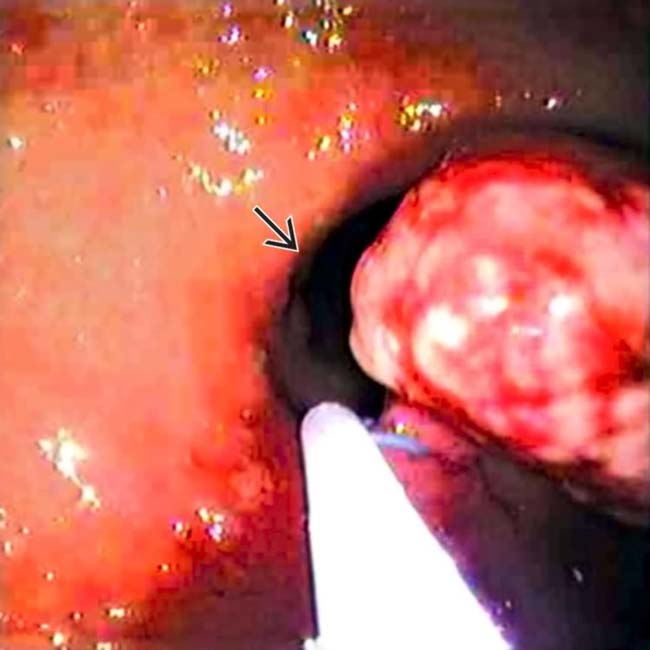
 .
.

 .
.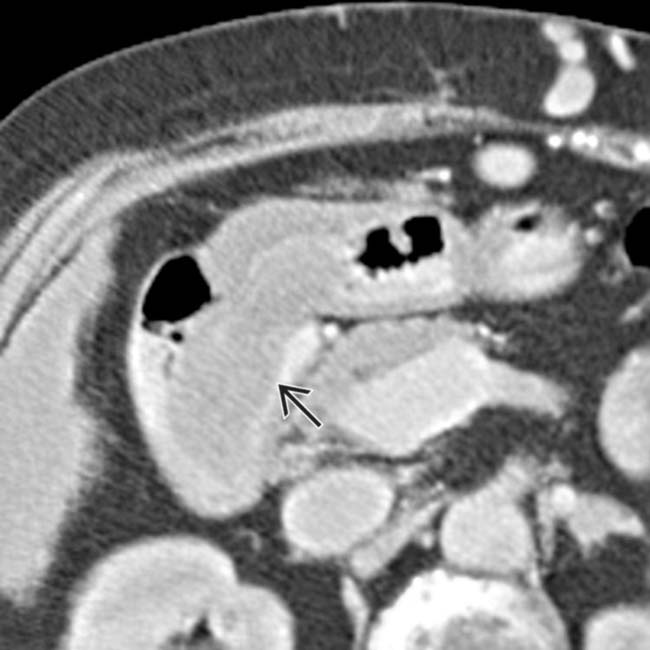
 prolapsed into the duodenum.
prolapsed into the duodenum.