[level-membership-for-pediatrics-category]
CHAPTER 17 Meconium Disease
Meconium Ileus
Step 1: Surgical Anatomy




Step 2: Preoperative Considerations
 The presentation varies depending on whether the obstruction is simple (uncomplicated) or complex (complicated).
The presentation varies depending on whether the obstruction is simple (uncomplicated) or complex (complicated).

Step 3: Treatment










Operative Considerations


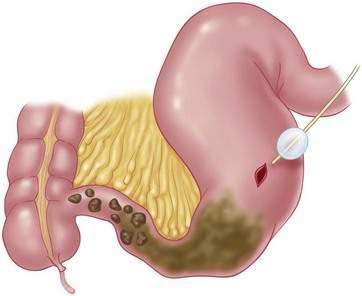
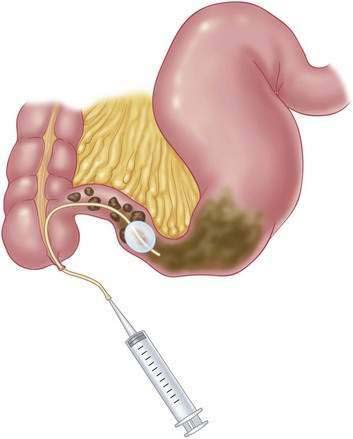
 A needle enterostomy involves multiple injections slanted through the wall of the bowel with a small-gauge needle to deliver saline, dilute Gastrografin, and/or 2% to 4% N-acetylcysteine. Once the meconium is liquefied by one or all of these substances, it can be manually passed into the colon and out the rectum.
A needle enterostomy involves multiple injections slanted through the wall of the bowel with a small-gauge needle to deliver saline, dilute Gastrografin, and/or 2% to 4% N-acetylcysteine. Once the meconium is liquefied by one or all of these substances, it can be manually passed into the colon and out the rectum.

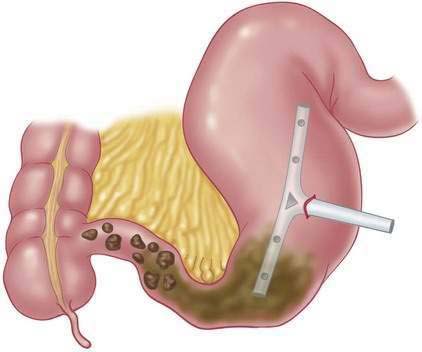
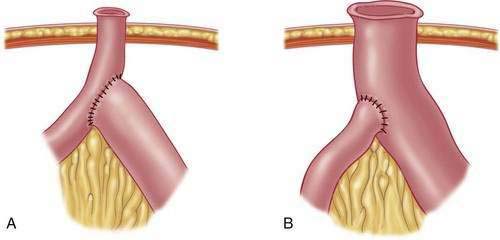
 If there is tenacious meconium that cannot be removed, or if there is a question of the ability of the enterotomy or appendiceal stump to heal, a T-tube (enterotomy) or Malecot (appendicostomy) can be placed to create a controlled fistula (Fig. 17-3). A 10 to 14 French T-tube is trimmed, and extra holes are cut before insertion. It is held in place by two pursestring sutures, and the bowel is sutured to the abdominal wall as well. In patients who have had a T-tube placed in the terminal ileum, daily irrigation with N-acetylcysteine is used to promote and maintain patency of the terminal ileum. Once pancreatic enzymes have been started and spontaneous defecation established, the tube can be removed 2 to 3 weeks after surgery. The fistula tract will then spontaneously close.
If there is tenacious meconium that cannot be removed, or if there is a question of the ability of the enterotomy or appendiceal stump to heal, a T-tube (enterotomy) or Malecot (appendicostomy) can be placed to create a controlled fistula (Fig. 17-3). A 10 to 14 French T-tube is trimmed, and extra holes are cut before insertion. It is held in place by two pursestring sutures, and the bowel is sutured to the abdominal wall as well. In patients who have had a T-tube placed in the terminal ileum, daily irrigation with N-acetylcysteine is used to promote and maintain patency of the terminal ileum. Once pancreatic enzymes have been started and spontaneous defecation established, the tube can be removed 2 to 3 weeks after surgery. The fistula tract will then spontaneously close.

Step 4: Postoperative Care
Step 5: Pearls and Pitfalls
Distal Intestinal Obstructive Syndrome
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
Step 3: Surgery
Other Meconium-Related Disorders
Meconium Plug Syndrome
Meconium Disease of Prematurity
Clatworthy HW, Howard WH. The meconium plug syndrome. Surgery. 1956;39:131-142.
Dimmitt RA, Moss RL. Meconium diseases in infants with very low birth weight. Semin Pediatr Surg. 2000;9(2):79-83.
Docherty JG, Zaki A, Coutts JAP, et al. Meconium ileus: a review 1972-1990. Br J Surg. 1992;79(6):571-573.
Escobar MA, Grosfeld JL, Burdick JJ, et al. Surgical considerations in cystic fibrosis: a 32-year evaluation of outcomes. Surgery. 2005;138(4):560-571. discussion 571-572
Meetze WH, Palazzolo VL, Bowling D, et al. Meconium passage in very-low-birth-weight infants. JPEN J Parenter Enteral Nutr. 1993;17(6):537-540.
Noblett HR. Treatment of uncomplicated meconium ileus by Gastrografin enema: A preliminary report. J Pediatr Surg. 1969;4:190-197.
Rescorla FJ, Grosfeld JL. Contemporary management of meconium ileus. World J Surg. 1993;17(3):318-325.
Rubinstein S, Moss R, Lewiston N. Constipation and meconium ileus equivalent in patients with cystic fibrosis. Pediatrics. 1986;78(3):473-479.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
CHAPTER 17 Meconium Disease
Meconium Ileus
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
The presentation varies depending on whether the obstruction is simple (uncomplicated) or complex (complicated).Step 3: Treatment
Operative Considerations
A needle enterostomy involves multiple injections slanted through the wall of the bowel with a small-gauge needle to deliver saline, dilute Gastrografin, and/or 2% to 4% N-acetylcysteine. Once the meconium is liquefied by one or all of these substances, it can be manually passed into the colon and out the rectum.[/not-level-membership-for-pediatrics-category]
