[level-membership-for-pediatrics-category]
CHAPTER 5 Esophageal Atresia with Tracheoesophageal Fistula
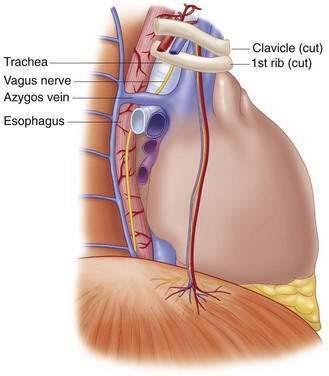
Step 1: Surgical Anatomy
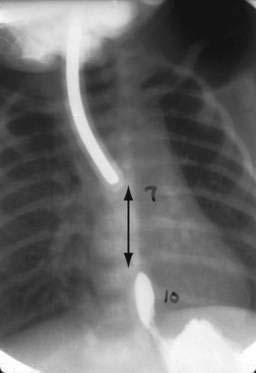
Step 2: Preoperative Considerations















Step 3: Operative Steps
Anesthetic Considerations
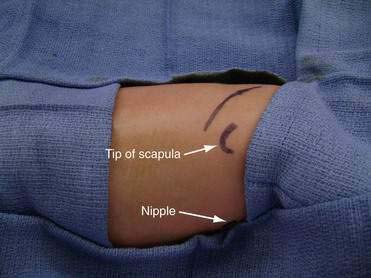
Positioning

Incision and Access
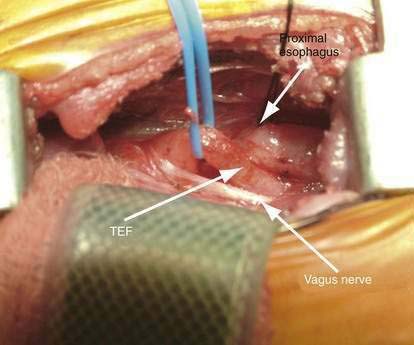
Division of the TEF and Mobilization of the Esophagus
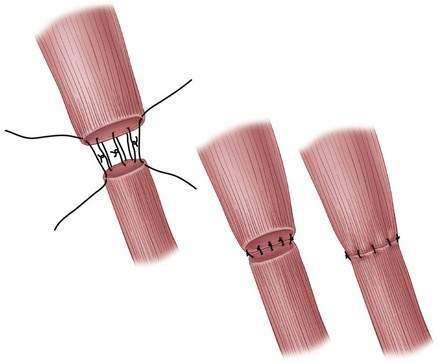
Anastomosis (Fig. 5-8)
Closing
Step 4: Postoperative Care
Step 5: Pearls and Pitfalls




Foker JE, Kendall TC, Carlton K, et al. A flexible approach to achieve a true primary repair for all infants with esophageal atresia. Semin Pediatr Surg. 2005;14:8-15.
Morrow SE, Ashcraft KW. Esophageal atresia. In: Ziegler MM, Azizkhan RG, Weber TR, editors. Operative pediatric surgery. New York: McGraw-Hill; 2003:349-354.
Raffensperger JG. Esophageal atresia and tracheoesophageal stenosis. In: Raffensperger JG, editor. Swenson’s pediatric surgery. 5th ed. Norwalk, CT: Appleton and Lange; 1990:697-717.
Ricketts RR, Luck SR, Raffensperger JG. Circular esophagomyotomy for primary repair of long-gap esophageal atresia. J Pediatr Surg. 1981;16:365-369.
Schwartz MZ. An improved technique for circular myotomy in long-gap esophageal atresia. J Pediatr Surg. 1983;18:833-834.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
CHAPTER 5 Esophageal Atresia with Tracheoesophageal Fistula
