[level-membership-for-anesthesiology-category]
CHAPTER 75 Laser Surgery and Operating Room Fires
2 What makes lasers behave differently from each other?
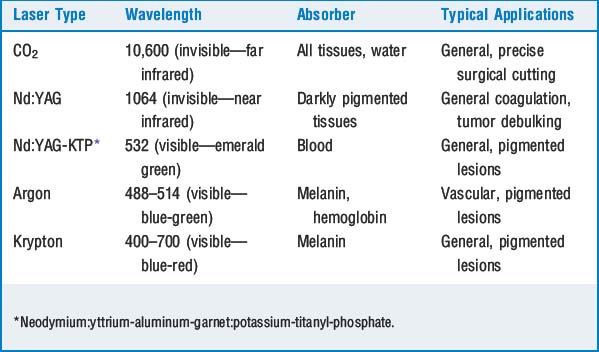
When excited, the source of the laser radiates light of a certain wavelength. The longer the wavelength, the more strongly it is absorbed by the tissue target, and the more shallow is the overall lasing effect. Conversely, the shorter the wavelength, the higher the energy, and the deeper the penetration of the laser light. For example, a carbon dioxide (CO2) laser has a longer wavelength and is absorbed almost entirely at the tissue surface. As a result, precise excision of superficial lesions is possible. Conversely, a neodymium:yttrium-aluminum-garnet (Nd: YAG) laser has a shorter wavelength, deeper penetration, and is useful for heating large tissue masses and tumor debulking (Table 75-1).
3 What are the hazards of lasers?





4 What are some unique airway considerations for the patient having laser surgery of the airway?
 Upper airway lesions: In laser resection of upper airway lesions, tracheal intubation is optional. Techniques that do not involve an endotracheal tube allow better visualization of the operative field by the surgeon and also remove potentially flammable materials from the airway. Clearly the airway is being shared by surgeon and anesthesiologist, and a discussion of the operative course before the procedure begins is important.
Upper airway lesions: In laser resection of upper airway lesions, tracheal intubation is optional. Techniques that do not involve an endotracheal tube allow better visualization of the operative field by the surgeon and also remove potentially flammable materials from the airway. Clearly the airway is being shared by surgeon and anesthesiologist, and a discussion of the operative course before the procedure begins is important.
5 Describe ventilation techniques commonly encountered during airway laser surgery
 Jet ventilation: In this technique the surgeon aims a high-velocity jet of O2 at the airway opening. The high flow of O2 entrains room air as a result of the Venturi effect, thus ventilating the lungs with a high volume of O2–air mixture. Ventilation is accomplished by attaching a suction catheter to wall O2 and a Sanderson-type jet injector. This apparatus is mounted to the operating laryngoscope. Sometimes the mass of the airway lesion makes this method impossible. If the jet stream is not aimed in the trachea, gastric dilation may occur. Barotrauma to the airway and subsequent pneumothorax are also risks and may in turn lead to mediastinal or subcutaneous air. An intravenous anesthetic is necessary for this procedure.
Jet ventilation: In this technique the surgeon aims a high-velocity jet of O2 at the airway opening. The high flow of O2 entrains room air as a result of the Venturi effect, thus ventilating the lungs with a high volume of O2–air mixture. Ventilation is accomplished by attaching a suction catheter to wall O2 and a Sanderson-type jet injector. This apparatus is mounted to the operating laryngoscope. Sometimes the mass of the airway lesion makes this method impossible. If the jet stream is not aimed in the trachea, gastric dilation may occur. Barotrauma to the airway and subsequent pneumothorax are also risks and may in turn lead to mediastinal or subcutaneous air. An intravenous anesthetic is necessary for this procedure.

6 What are the three essential components necessary to create an operating room fire?
8 What strategies can reduce the incidence of airway fires?
 Laser-resistant endotracheal tubes should be chosen. The cuffs should be filled with saline, not air, and it is also recommended that the saline contain a small quantity of methylene blue to help identify rupture of the cuff, should this happen (as in an airway laser procedure). Many laser specialty tubes already have dye crystals within the cuffs. Cuffed tubes are also preferable to uncuffed tubes.
Laser-resistant endotracheal tubes should be chosen. The cuffs should be filled with saline, not air, and it is also recommended that the saline contain a small quantity of methylene blue to help identify rupture of the cuff, should this happen (as in an airway laser procedure). Many laser specialty tubes already have dye crystals within the cuffs. Cuffed tubes are also preferable to uncuffed tubes.


10 Should an airway fire occur, what are the recommended practices for its management?











1. American Society of Anesthesiologists. Practice advisory for the prevention and management of operating room fires. Anesthesiology. 2008;108:786-801.
2. Rampil I.J. Anesthesia for laser surgery. In: Miller R.D., editor. Miller’s anesthesia. ed 6. Philadelphia: Elsevier Churchill Livingstone; 2005:2573-2587.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
CHAPTER 75 Laser Surgery and Operating Room Fires
2 What makes lasers behave differently from each other?
When excited, the source of the laser radiates light of a certain wavelength. The longer the wavelength, the more strongly it is absorbed by the tissue target, and the more shallow is the overall lasing effect. Conversely, the shorter the wavelength, the higher the energy, and the deeper the penetration of the laser light. For example, a carbon dioxide (CO2) laser has a longer wavelength and is absorbed almost entirely at the tissue surface. As a result, precise excision of superficial lesions is possible. Conversely, a neodymium:yttrium-aluminum-garnet (Nd: YAG) laser has a shorter wavelength, deeper penetration, and is useful for heating large tissue masses and tumor debulking (Table 75-1).
