[level-membership-for-anesthesiology-category]
CHAPTER 66 Epidural Analgesia and Anesthesia
1 Where is the epidural space? Describe the relevant anatomy






Beyond the epidural space lie the spinal meninges and CSF. The epidural space has its widest point (5 mm) at L2. In addition to the traversing nerve roots, it contains fat, lymphatics, and an extensive venous plexus. Superiorly the space extends to the foramen magnum, where dura is fused to the base of the skull. Caudally it ends at the sacral hiatus. The epidural space can be entered in the cervical, thoracic, lumbar, or sacral regions to provide anesthesia. In pediatric patients the caudal epidural approach is commonly used (see Question 3).



4 What are the advantages of using epidural anesthesia vs. general anesthesia?












6 What are the advantages of epidural anesthesia over spinal anesthesia?





7 What are the disadvantages of epidural compared with spinal anesthesia?



8 What factors should the anesthesiologist address in the preoperative assessment before performing an epidural anesthetic? Should special laboratory tests be performed?
 History
History
















9 Describe the technique for performing a lumbar epidural anesthetic










10 Are there any contraindications to epidural anesthesia?













11 What are the potential complications of epidural anesthesia? Can they be anticipated or prevented?
 Hypotension caused by sympathetic blockade, which may be prevented by fluid preload and patient positioning.
Hypotension caused by sympathetic blockade, which may be prevented by fluid preload and patient positioning. Intravascular injection of local anesthetic, which can be prevented by aspirating the catheter for blood, injecting a marker such as epinephrine that will cause tachycardia if injected into a vessel, and using incremental dosing (no more than 5 ml at a time). If an intravascular injection occurs:
Intravascular injection of local anesthetic, which can be prevented by aspirating the catheter for blood, injecting a marker such as epinephrine that will cause tachycardia if injected into a vessel, and using incremental dosing (no more than 5 ml at a time). If an intravascular injection occurs:
 Stop convulsions with an induction agent or rapid-acting anticonvulsant. Intubate the trachea, if necessary, for ventilation and airway protection.
Stop convulsions with an induction agent or rapid-acting anticonvulsant. Intubate the trachea, if necessary, for ventilation and airway protection.




12 What physiologic changes should be expected after successful initiation of an epidural anesthetic?







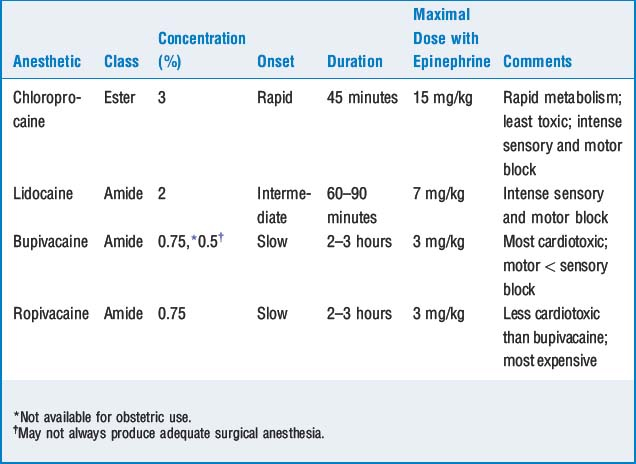
13 How does one choose which local anesthetic to use?
The choice of local anesthetic is usually based on the onset, duration, safety profile, and the special clinical characteristics of the patient and surgical procedure (Table 66-1).
14 Why is epinephrine sometimes combined with the local anesthetic? Should it be included in all cases?




15 When should opioids be included in the epidural anesthetic?
KEY POINTS: Epidural Analgesia and Anesthesia 
16 Why can some patients with epidural blocks move around and even walk, whereas others have a dense motor block?
18 How do you determine the level of anesthesia needed for different types of surgeries? What is a segmental block? When is it used?
19 How do you determine the amount of local anesthetic solution used for different procedures? What factors affect spread in the epidural space?










[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
CHAPTER 66 Epidural Analgesia and Anesthesia
1 Where is the epidural space? Describe the relevant anatomy
Beyond the epidural space lie the spinal meninges and CSF. The epidural space has its widest point (5 mm) at L2. In addition to the traversing nerve roots, it contains fat, lymphatics, and an extensive venous plexus. Superiorly the space extends to the foramen magnum, where dura is fused to the base of the skull. Caudally it ends at the sacral hiatus. The epidural space can be entered in the cervical, thoracic, lumbar, or sacral regions to provide anesthesia. In pediatric patients the caudal epidural approach is commonly used (see Question 3).
4 What are the advantages of using epidural anesthesia vs. general anesthesia?
6 What are the advantages of epidural anesthesia over spinal anesthesia?
7 What are the disadvantages of epidural compared with spinal anesthesia?
8 What factors should the anesthesiologist address in the preoperative assessment before performing an epidural anesthetic? Should special laboratory tests be performed?
History
