[level-membership-for-surgery-category]
Chapter 18 Biologic Mesh Choices for Surgical Repair
1 Indications for the Use of Biologic Mesh Materials
 The major indication for the use of biologic meshes during abdominal wall surgery is improved wound healing. This most often translates into the minimization of wound complications. Studies have reported wound infection rates of 4% to 16% after incisional ventral hernia repair. The application of synthetic mesh to reinforce abdominal wall repairs significantly reduced recurrence rates, but it introduced an increased risk of complicated wound infections, synthetic mesh infections and erosion into the bowel. Level one data find that recurrence rate and wound infection are related, in that a postoperative wound infection significantly increases the incidence of recurrent incisional hernia. Another inherent limitation with synthetic meshes is shrinkage. It is well measured now in animal models and with human explants that synthetic meshes lose on the average 20% of their surface area following implantation. This is believed to contribute to high hernia recurrence rates. The era of managing traumatized patients with open abdomens expanded the use of biologic mesh based abdominal wall reconstruction. Here there was concern for wound contamination and exposure of synthetic prostheses to the abdominal viscera. Tenuous or insufficient skin coverage also is suggested as an indication for the use of a biologic mesh during abdominal wall repair.
The major indication for the use of biologic meshes during abdominal wall surgery is improved wound healing. This most often translates into the minimization of wound complications. Studies have reported wound infection rates of 4% to 16% after incisional ventral hernia repair. The application of synthetic mesh to reinforce abdominal wall repairs significantly reduced recurrence rates, but it introduced an increased risk of complicated wound infections, synthetic mesh infections and erosion into the bowel. Level one data find that recurrence rate and wound infection are related, in that a postoperative wound infection significantly increases the incidence of recurrent incisional hernia. Another inherent limitation with synthetic meshes is shrinkage. It is well measured now in animal models and with human explants that synthetic meshes lose on the average 20% of their surface area following implantation. This is believed to contribute to high hernia recurrence rates. The era of managing traumatized patients with open abdomens expanded the use of biologic mesh based abdominal wall reconstruction. Here there was concern for wound contamination and exposure of synthetic prostheses to the abdominal viscera. Tenuous or insufficient skin coverage also is suggested as an indication for the use of a biologic mesh during abdominal wall repair.
 The growing popularity of major reconstructive procedures for large ventral hernias also expanded the use of biologic meshes. The perceived need for reinforcement following component separation procedures and the concern for the implantation of synthetic materials into these large surface area wounds led to this adaptation of biologic mesh. Clinical studies have supported reduced recurrence rates using mesh reinforcement during component separation.
The growing popularity of major reconstructive procedures for large ventral hernias also expanded the use of biologic meshes. The perceived need for reinforcement following component separation procedures and the concern for the implantation of synthetic materials into these large surface area wounds led to this adaptation of biologic mesh. Clinical studies have supported reduced recurrence rates using mesh reinforcement during component separation.2 Tissue Sources for Biologic Mesh Materials (Table 18-1)
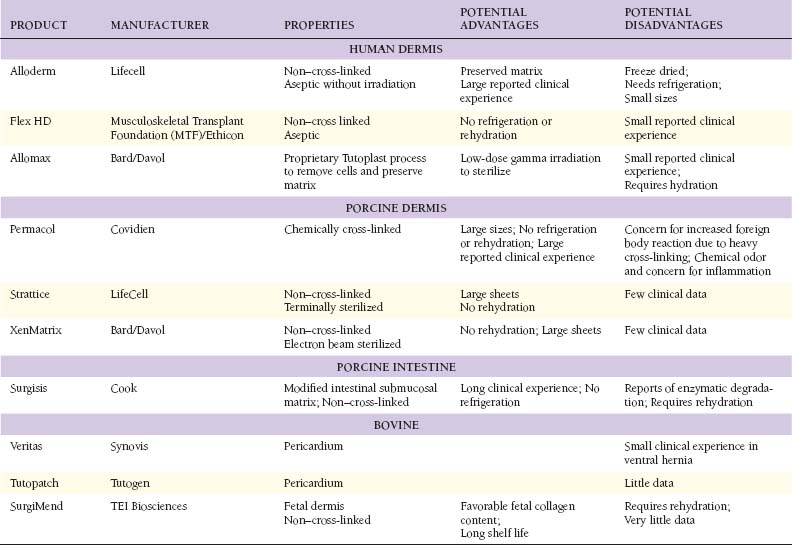
 The application of biologic materials to abdominal wall repair began with autologous source material. Tensor fascia lata (TFL) has the widest experience. De-epithelialized autologous dermis also has been used. Muscle flaps and now even composite tissue transfers, both pedicle based and free flaps, have been described. Autologous small bowel and omentum also are reported as tissue sources for abdominal wall repair. Donor site morbidity is the obvious limitation of autologous biologic tissue sources. There are no large studies of TFL or autologous dermis in abdominal wall repair, and the long-term durability, especially when used as bridging repair, is not known.
The application of biologic materials to abdominal wall repair began with autologous source material. Tensor fascia lata (TFL) has the widest experience. De-epithelialized autologous dermis also has been used. Muscle flaps and now even composite tissue transfers, both pedicle based and free flaps, have been described. Autologous small bowel and omentum also are reported as tissue sources for abdominal wall repair. Donor site morbidity is the obvious limitation of autologous biologic tissue sources. There are no large studies of TFL or autologous dermis in abdominal wall repair, and the long-term durability, especially when used as bridging repair, is not known. The need for more readily available biologic reconstructive matrices and the limitation of autologous tissue donor site morbidity led to the development of off-the-shelf human allograft sources for abdominal wall reconstruction. To date, this has been dominated by human dermal allografts. Although early results have been good, there is an inherent limitation in the need for human tissue banking and the risk of transmission of infectious disease. Before processing, potential donors undergo screening that includes a medical and social history review, physical examination and serologic testing to minimize the risk of disease transmission. Donor tissue that passes rigorous screening then undergoes physical and chemical processing to further reduce the risk of disease transmission before implantation. Occasionally, social and cultural restrictions may preclude the application of human tissue sources to specific patient groups.
The need for more readily available biologic reconstructive matrices and the limitation of autologous tissue donor site morbidity led to the development of off-the-shelf human allograft sources for abdominal wall reconstruction. To date, this has been dominated by human dermal allografts. Although early results have been good, there is an inherent limitation in the need for human tissue banking and the risk of transmission of infectious disease. Before processing, potential donors undergo screening that includes a medical and social history review, physical examination and serologic testing to minimize the risk of disease transmission. Donor tissue that passes rigorous screening then undergoes physical and chemical processing to further reduce the risk of disease transmission before implantation. Occasionally, social and cultural restrictions may preclude the application of human tissue sources to specific patient groups.
3 Biologic Mesh Modification and Processing
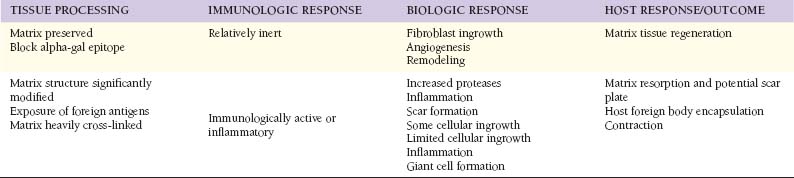
 The use of biologic allografts and xenografts for soft tissue repair required the development of processing techniques that allowed for the removal of immunogenic cells, while preserving a functional biologic matrix. This remnant biologic matrix is constructed primarily of collagen, and depending on the degree of preservation of the native structure, maintains measurable biologic function even in the acellularized state.
The use of biologic allografts and xenografts for soft tissue repair required the development of processing techniques that allowed for the removal of immunogenic cells, while preserving a functional biologic matrix. This remnant biologic matrix is constructed primarily of collagen, and depending on the degree of preservation of the native structure, maintains measurable biologic function even in the acellularized state.

 Allografts and xenografts vary in the degree of terminal sterilization. Some methods limit terminal sterilization, using instead aseptic techniques. It is believed that this ensures preservation of extracellular matrix structure with improved biologic function following implantation. Other biologic mesh materials undergo true terminal sterilization, as with low-dose gamma irradiation. It is believed that this step may be important to minimizing infectious complications.
Allografts and xenografts vary in the degree of terminal sterilization. Some methods limit terminal sterilization, using instead aseptic techniques. It is believed that this ensures preservation of extracellular matrix structure with improved biologic function following implantation. Other biologic mesh materials undergo true terminal sterilization, as with low-dose gamma irradiation. It is believed that this step may be important to minimizing infectious complications.4 Mechanism of Action of Biologic Meshes (Table 18-2)
 The primary function of soft tissue prostheses, whether synthetic or biologic meshes, is to provide immediate and long-term mechanical stability to the abdominal wall reconstruction. Level one evidence derived from a randomized, controlled trial found that the use of a reinforcing mesh prosthesis reduces the incisional hernia recurrence rate by 50%. The major risk of synthetic mesh implants is the permanent foreign body reaction, infection, encapsulation, extrusion, and erosion. There is now experimental and clinical evidence that biologic meshes may be repopulated with endothelial cells, revascularized and then incorporated into an abdominal wall reconstruction. It is the early establishment of a blood supply that is believed to establish improved resistance to infection. Further, as a blood supply is restored, other cells involved in tissue repair like inflammatory cells and fibroblasts may be recruited to promote more normal wound healing, and ideally, tissue regeneration.
The primary function of soft tissue prostheses, whether synthetic or biologic meshes, is to provide immediate and long-term mechanical stability to the abdominal wall reconstruction. Level one evidence derived from a randomized, controlled trial found that the use of a reinforcing mesh prosthesis reduces the incisional hernia recurrence rate by 50%. The major risk of synthetic mesh implants is the permanent foreign body reaction, infection, encapsulation, extrusion, and erosion. There is now experimental and clinical evidence that biologic meshes may be repopulated with endothelial cells, revascularized and then incorporated into an abdominal wall reconstruction. It is the early establishment of a blood supply that is believed to establish improved resistance to infection. Further, as a blood supply is restored, other cells involved in tissue repair like inflammatory cells and fibroblasts may be recruited to promote more normal wound healing, and ideally, tissue regeneration.
5 Reported Clinical Results with Biologic Meshes
 The choice of biologic mesh material may be based on a variety of considerations, including characteristics of the patient and abdominal wall defect, surgeon familiarity with the material, and cost. The risk for surgical wound complication and subsequent infection may determine the selection of a synthetic versus a biologic repair material. On the balance, the biologic mesh material should provide sustained mechanical function resulting in an acceptable recurrence rate with resistance to wound infection, especially when compared to the synthetic counter parts.
The choice of biologic mesh material may be based on a variety of considerations, including characteristics of the patient and abdominal wall defect, surgeon familiarity with the material, and cost. The risk for surgical wound complication and subsequent infection may determine the selection of a synthetic versus a biologic repair material. On the balance, the biologic mesh material should provide sustained mechanical function resulting in an acceptable recurrence rate with resistance to wound infection, especially when compared to the synthetic counter parts.






Breuing K., Butler C.E., Ferzoco S., et al. Incisional ventral hernias: Review of the literature and recommendations regarding the grading and technique of repair. Surgery. 2010;148(3):544-558.
Diaz J.J.Jr., Conquest A.M., Ferzoco S.J., Vargo D., Miller P., Wu Y.C., et al. Multi-institutional experience using human acellular dermal matrix for ventral hernia repair in a compromised surgical field. Arch Surg. 2009 Mar;144(3):209-215.
Espinosa-de-Los-Monteros A., de la Torre J.I., Marrero I., Andrades P., Davis M.R., Vasconez L.O. Utilization of human cadaveric acellular dermis for abdominal hernia reconstruction. Ann Plast Surg. 2007 Mar;58(3):264-267.
Franz M.G. The biology of hernia formation. Surg Clin North Am. 2008 Feb;88(1):1-15. vii
Gray S.H., Vick C.C., Graham L.A., Finan K.R., Neumayer L.A., Hawn M.T. Risk of complications from enterotomy or unplanned bowel resection during elective hernia repair. Arch Surg. 2008 Jun;143(6):582-586.
Halm J.A., de Wall L.L., Steyerberg E.W., Jeekel J., Lange J.F. Intraperitoneal polypropylene mesh hernia repair complicates subsequent abdominal surgery. World J Surg. 2007 Feb;31(2):423-429.
Luijendijk R.W., Hop W.C.J., van den Tol P., de Lange D.C.D., Braaksma M.M.J., Ijzermans J.N.M., et al. A comparison of suture repair with mesh repair for incisional hernia. New England Journal of Medicine. 2000 Aug 10;343(6):392-398.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Chapter 18 Biologic Mesh Choices for Surgical Repair
1 Indications for the Use of Biologic Mesh Materials
The major indication for the use of biologic meshes during abdominal wall surgery is improved wound healing. This most often translates into the minimization of wound complications. Studies have reported wound infection rates of 4% to 16% after incisional ventral hernia repair. The application of synthetic mesh to reinforce abdominal wall repairs significantly reduced recurrence rates, but it introduced an increased risk of complicated wound infections, synthetic mesh infections and erosion into the bowel. Level one data find that recurrence rate and wound infection are related, in that a postoperative wound infection significantly increases the incidence of recurrent incisional hernia. Another inherent limitation with synthetic meshes is shrinkage. It is well measured now in animal models and with human explants that synthetic meshes lose on the average 20% of their surface area following implantation. This is believed to contribute to high hernia recurrence rates. The era of managing traumatized patients with open abdomens expanded the use of biologic mesh based abdominal wall reconstruction. Here there was concern for wound contamination and exposure of synthetic prostheses to the abdominal viscera. Tenuous or insufficient skin coverage also is suggested as an indication for the use of a biologic mesh during abdominal wall repair. The growing popularity of major reconstructive procedures for large ventral hernias also expanded the use of biologic meshes. The perceived need for reinforcement following component separation procedures and the concern for the implantation of synthetic materials into these large surface area wounds led to this adaptation of biologic mesh. Clinical studies have supported reduced recurrence rates using mesh reinforcement during component separation.2 Tissue Sources for Biologic Mesh Materials (Table 18-1)
The application of biologic materials to abdominal wall repair began with autologous source material. Tensor fascia lata (TFL) has the widest experience. De-epithelialized autologous dermis also has been used. Muscle flaps and now even composite tissue transfers, both pedicle based and free flaps, have been described. Autologous small bowel and omentum also are reported as tissue sources for abdominal wall repair. Donor site morbidity is the obvious limitation of autologous biologic tissue sources. There are no large studies of TFL or autologous dermis in abdominal wall repair, and the long-term durability, especially when used as bridging repair, is not known. The need for more readily available biologic reconstructive matrices and the limitation of autologous tissue donor site morbidity led to the development of off-the-shelf human allograft sources for abdominal wall reconstruction. To date, this has been dominated by human dermal allografts. Although early results have been good, there is an inherent limitation in the need for human tissue banking and the risk of transmission of infectious disease. Before processing, potential donors undergo screening that includes a medical and social history review, physical examination and serologic testing to minimize the risk of disease transmission. Donor tissue that passes rigorous screening then undergoes physical and chemical processing to further reduce the risk of disease transmission before implantation. Occasionally, social and cultural restrictions may preclude the application of human tissue sources to specific patient groups.3 Biologic Mesh Modification and Processing
The use of biologic allografts and xenografts for soft tissue repair required the development of processing techniques that allowed for the removal of immunogenic cells, while preserving a functional biologic matrix. This remnant biologic matrix is constructed primarily of collagen, and depending on the degree of preservation of the native structure, maintains measurable biologic function even in the acellularized state.[/not-level-membership-for-surgery-category]
