CASE 96
History: A 46-year-old man is undergoing investigations for an abnormal heartbeat.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figure? (Choose all that apply.)
2. Which of the following statements regarding primary hemochromatosis is true?
A. Disease more commonly affects male patients.
B. Inheritance is X-linked recessive.
C. Iron deposition is visible on imaging in the liver and spleen.
3. What is the gold standard for the measurement of the iron deposition in the liver?
4. What is the most serious complication of hemochromatosis?
ANSWERS
CASE 96
Hemochromatosis
1. C and D
2. A
3. B
4. C
References
Gandon Y, Guyader D, Heautot JF, et al: Hemochromatosis: diagnosis and quantification of liver iron with gradient-echo MR imaging. Radiology. 1994;193:533–538.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 207.
Comment
Hemochromatosis is an inherited disorder of increased iron absorption from dietary food sources, which over time leads to overload of iron deposition in different sites within the body. This iron deposition leads to cirrhosis, insulin-dependent diabetes, arthropathy, and cardiac problems. In hereditary or primary hemochromatosis, the liver is the main organ of iron deposition initially. Hemosiderosis or secondary hemochromatosis can develop in patients who receive multiple blood transfusions over time. Other causes of increased iron body stores can be from thalassemia with increased demand for iron in the bone marrow secondary to ineffective erythropoiesis and also hemolytic anemias.
Bantu siderosis is a condition found in parts of Africa resulting from abnormal iron deposition in the liver. It is most commonly found in those with an increased predisposition for iron absorption and a thirst for homemade beer. This beer, brewed locally, contains a large amount of iron.
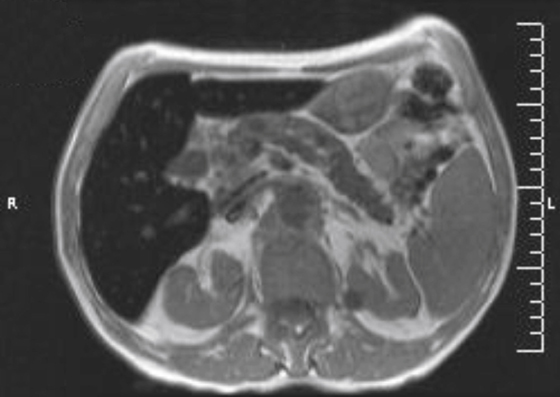
Iron deposition can be detected and quantified by MRI. Iron results in signal loss, particularly on T2-weighted sequences (long TE), including gradient echoes, which are the best sequence for assessing iron (see figure).
Hemochromatosis and hemosiderosis cause the liver to increase in density owing to the accumulation and metabolism of iron in the liver. Hemochromatosis is a primary disorder of iron metabolism. Hemosiderosis occurs in a patient who has received multiple blood transfusions or has had a high turnover of blood, such as with hemolytic anemia.
Relative density on an unenhanced CT scan of the liver should raise the question of the use of the antiarrhythmic drug amiodarone. This drug causes the liver to increase in density owing to its accumulation and metabolism in the liver and the fact that amiodarone contains iodine. Increased liver density may be common inpatients taking this useful medication, but actual hepatotoxicity is uncommon.
Other considerations for a high-density liver include Wilson’s disease, a disease of copper metabolism; malfunction is rare but can result in a dense liver. Older patients who received Thorotrast in the 1960s and who are still alive (there are very few today) have increased density of liver and spleen. Patients treated with intramuscular gold for rheumatoid arthritis might have such a finding as well as those with some of the glycogen storage diseases.






