CASE 94
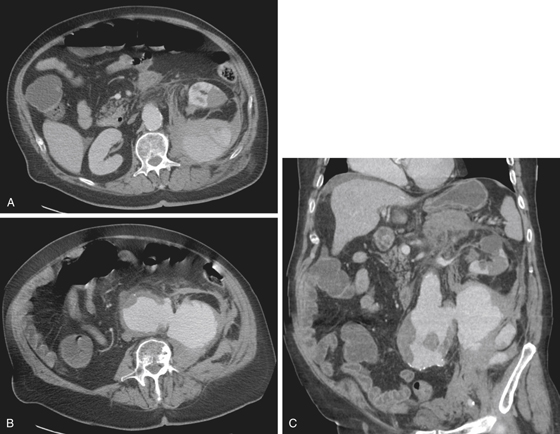
History: A 76-year-old man presents with left flank pain.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. Which of the following statements regarding aortic aneurysm is true?
A. Male and female patients are equally affected.
B. It is most commonly located just above the bifurcation.
C. Smoking is the major risk factor for aneurysm formation.
D. Aneurysm is defined as aortic dilation more than 2 cm diameter.
3. What is the most common clinical presentation of a patient with an abdominal aortic aneurysm?
4. What is the preferred imaging modality for screening for aortic aneurysm?
ANSWERS
CASE 94
Abdominal Aortic Aneurysm
1. A, B, and D
2. C
3. A
4. B
References
LaRoy LL, Cormier PJ, Matalon TA, et al: Imaging of abdominal aortic aneurysms. Am J Roentgenol. 1989;152:785–792.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 138.
Comment
Abdominal aneurysms are relatively common in elderly patients. Whites are more likely to have it and men are affected seven times more often than women. The aorta comprises three layers: intima, media, and adventitia. Abdominal aortic aneurysms (AAAs) occur over long periods of time during which medial degeneration takes place, resulting in a gradual dilation of the vessel.
However, not all AAAs are caused by degenerative disease. In a small percentage of cases (3% to 5%), the mycotic aneurysm results from the hematogenous spread of bacteria. Most AAAs are fusiform in shape and are located below the renal arteries and the bifurcation. Some extend into the iliac vessels.
Most AAAs are asymptomatic until they suddenly expand, leak, rupture, or compromise renal or enteric vessels. Almost two thirds of patients with sudden rupture die from rapid cardiovascular collapse before reaching the hospital. CT usually reveals a large dilated abdominal aorta with varying degrees of intramural thrombus. Care should be taken to evaluate for dissection, blood leakage, and quality of kidney and bowel perfusion. Pain associated with AAA can be misdiagnosed, because the classic presentation of tachycardia, hypotension, and a pulsatile mass on physical diagnosis is, as most classical presentations, not the most common. Often these patients present with flank pain and kidney stones. multidetector CT protocols are performed looking for the offending calculi. In the event of an elderly patient presenting with flank pain with no obvious urologic source, with or without an AAA, the possibility of dissection should not be overlooked.
Uncommon causes of AAA include Marfan’s syndrome and Ehlers-Danlos disease.






