CASE 94


1. What should be included in the differential diagnosis? (Choose all that apply.)
A. Metastasis
B. Lymphoma
C. Myxoma
D. Angiosarcoma
2. What is the most common mass in the heart?
A. Thrombus
B. Myxoma
C. Metastasis
D. Angiosarcoma
3. Which imaging feature suggests that this mass is a tumor rather than a thrombus?
A. Enhancement
B. Dark signal on steady-state free precession images
C. Size
4. Which of the following malignant features is depicted on MRI?
A. Extension outside the heart
ANSWERS
Reference
Randhawa K, Ganeshan A, Hoey ET. Magnetic resonance imaging of cardiac tumors: part 2, malignant tumors and tumor-like conditions. Curr Probl Diagn Radiol. 2011;40(4):169–179.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 277–278.
Comment
Etiology and Diagnosis
Approximately 98% of cardiac tumors are secondary tumors, most commonly from direct extension (lymphoma or metastatic breast or lung carcinoma) or hematogenous spread (melanoma, lung or breast carcinoma). Other primary malignant tumors are rare and include angiosarcoma, rhabdomyosarcoma, leiomyosarcoma, liposarcoma, and lymphoma. In patients with renal cell carcinoma, the tumor can enter the right atrium via the inferior vena cava. When the patient has a known malignant neoplasm elsewhere in the body, the most likely diagnosis is secondary tumor involvement of the heart. Definitive diagnosis can be made by endomyocardial or open biopsy.
Imaging
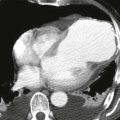
MRI shows tumor size and location as well as cardiac function. Contrast-enhanced sequences can delineate tumor margins and invasion into adjacent structures. The presence of enhancement does not signify malignancy—benign tumors also enhance. Features that suggest a primary malignant cardiac tumor include irregular or ill-defined margination, invasiveness, extension outside the heart, involvement of more than one chamber, central necrosis, large pericardial effusion, and lung nodules, which also raise the possibility of metastases. The patient in this case had non-Hodgkin lymphoma involving the mediastinum and extending into the heart (Figs. A and B).