Procedure 91 Treatment of Mucous Cysts of the Distal Interphalangeal Joint




Examination/Imaging
Clinical Examination
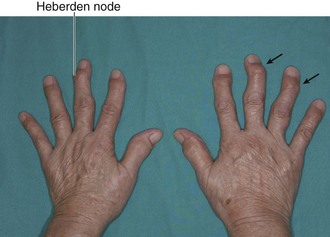
 A mucous cyst is a degenerative cyst of the DIP joint arising as a result of osteoarthritis. It usually occurs between the fifth and seventh decades of life, and patients have DIP joint osteoarthritis including Heberden nodes (Fig. 91-2).
A mucous cyst is a degenerative cyst of the DIP joint arising as a result of osteoarthritis. It usually occurs between the fifth and seventh decades of life, and patients have DIP joint osteoarthritis including Heberden nodes (Fig. 91-2).
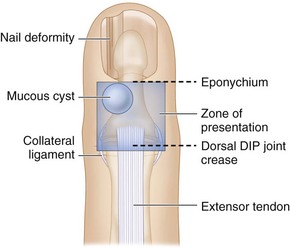
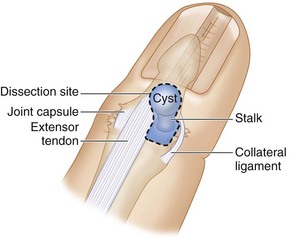
 The cyst may present on the dorsum at the level of the DIP joint on either side between the extensor tendon and the collateral ligament or under the eponychium to cause longitudinal grooving of the nail plate (Fig. 91-3).
The cyst may present on the dorsum at the level of the DIP joint on either side between the extensor tendon and the collateral ligament or under the eponychium to cause longitudinal grooving of the nail plate (Fig. 91-3).


Surgical Anatomy
 The mucous cyst originates from the DIP joint in relation to one of the osteophytes, and the stalk of the cyst passes between the collateral ligament and the extensor insertion to present on the dorsum of the DIP joint. Occasionally, the stalk can connect with another mucous cyst on the opposite side of the DIP joint. This cyst may not be clinically obvious (occult cyst), and the entire DIP joint should be examined during surgery.
The mucous cyst originates from the DIP joint in relation to one of the osteophytes, and the stalk of the cyst passes between the collateral ligament and the extensor insertion to present on the dorsum of the DIP joint. Occasionally, the stalk can connect with another mucous cyst on the opposite side of the DIP joint. This cyst may not be clinically obvious (occult cyst), and the entire DIP joint should be examined during surgery.
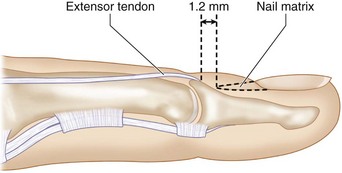
 The terminal extensor insertion is about 1.2 mm from the proximal edge of the nail matrix (Fig. 91-5).
The terminal extensor insertion is about 1.2 mm from the proximal edge of the nail matrix (Fig. 91-5).

Exposures


Procedure
Step 1: Mobilization of Cyst


Step 2: Removal of the Cyst
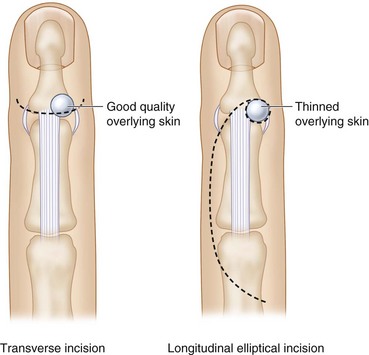
 The cyst is excised en-mass and includes any thinned overlying skin, the cyst and the stalk, and all soft tissue between the extensor tendon and collateral ligament (synovium and joint capsule). (Fig. 91-7 depicts the soft tissue zone that needs to be excised in the dotted line.)
The cyst is excised en-mass and includes any thinned overlying skin, the cyst and the stalk, and all soft tissue between the extensor tendon and collateral ligament (synovium and joint capsule). (Fig. 91-7 depicts the soft tissue zone that needs to be excised in the dotted line.)

Step 2 Pearls
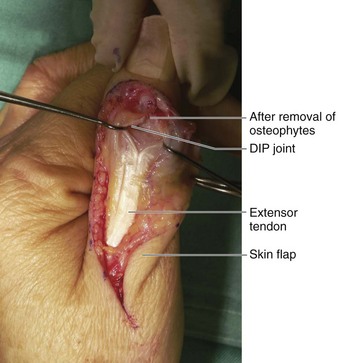
It is important to remove all synovium to allow a clear visualization of the DIP joint.
Both sides of the extensor tendon must be examined for any occult cysts.
It is preferable to leave behind a portion of the cyst wall that is in close relation to the nail bed rather than risk injury to the nail bed from an aggressive débridement.

Step 4: Flap Elevation

Step 5: Skin Closure
 The tourniquet is released and hemostasis secured.
The tourniquet is released and hemostasis secured.
 The flap is advanced into the defect (Fig. 91-9) and sutured with a few 5-0 Ethilon sutures.
The flap is advanced into the defect (Fig. 91-9) and sutured with a few 5-0 Ethilon sutures.

Step 5 Pearls
It is better to close the skin loosely and leave any residual skin defects to heal by secondary intention instead of attempting a watertight closure.
A Xeroform dressing with overlying gauze is applied as a wick to absorb any residual blood. A volar finger splint is applied to keep the DIP joint straight.




