[level-membership-for-gastroenterology-and-hepatology-category]CASE 91
History: A 63-year-old woman presents with perineal soiling.
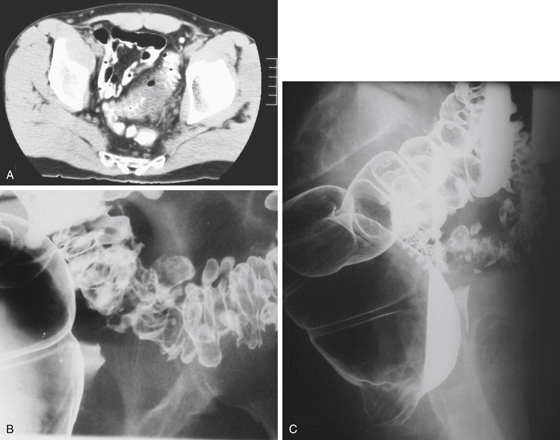
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. Where is the fistula shown in figures 2 and 3 extending to?
3. Which statement about colonic fistulas to the urogenital tract is true?
A. The most common fistula site is colovaginal.
B. The fistula is usually directly visualized on CT.
C. Sigmoidoscopy usually shows the fistula.
D. The most common cause is colonic diverticulitis.
E. Colovesical fistulas occur more commonly in female patients.
4. What is the worldwide most common cause of rectovaginal fistulas?
ANSWERS
CASE 91
Colovaginal Fistula
1. A, B, and D
2. E
3. D
4. A
References
Cho KC, Morehouse HT, Alterman DD, Thornhill BA. Sigmoid diverticulitis: diagnostic role of CT. Comparison with barium enema studies. Radiology. 1990;176:111–115.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 303.
Comment
A fistula is defined as an abnormal tract extending from one mucosa-lined organ into the mucosal surface of another organ. The possible types include enteroenteric (between two loops of bowel), enterovesical (bowel to bladder), enterovaginal, and enterocutaneous, among others. A sinus is also a tract communicating with bowel, but it ends blindly or in a cavity that is not normally lined with mucosa.
In the colon, diverticulitis is the most common cause of fistulas in industrialized society, such as seen in this case; figures 2 and 3 show a tract developing from inflamed sigmoid colon directing toward the vagina. Other inflammatory conditions also lead to the formation of numerous fistulas. Crohn’s disease is a relatively common and well-known cause of fistula formation in the gastrointestinal tract. Fistula formation occurs between adjacent loops of bowel, as well as with other structures. Some infections that can produce fistulas are tuberculosis and actinomycosis. This chronic inflammatory process ulcerates and produces a variety of unusual fistulas. Fistulas can form as a complication of surgery, typically at an anastomotic site that dehisces. Malignancy can also result in fistulous formation, especially if it is fairly extensive or is already being treated (leading to necrosis) before the fistula occurs. Radiation is a well-known cause of fistula development; this complication results from microvascular ischemic changes and fibrosis and matting together of organs.
Fluoroscopic studies (cystogram, contrast enema, small bowel study, even vaginogram) are valuable for confirming and defining the anomalous communication. Evaluation of fistulas can be quite difficult. Often, contrast material travels in only one direction through a fistula. Also, the fistula must be open at the time of the study, or it cannot be demonstrated. CT and MRI are good modalities for revealing the presence of the underlying condition leading to the fistula (see figures).
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 91
History: A 63-year-old woman presents with perineal soiling.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. Where is the fistula shown in figures 2 and 3 extending to?
3. Which statement about colonic fistulas to the urogenital tract is true?
A. The most common fistula site is colovaginal.
B. The fistula is usually directly visualized on CT.
C. Sigmoidoscopy usually shows the fistula.
D. The most common cause is colonic diverticulitis.
[/not-level-membership-for-gastroenterology-and-hepatology-category]
