
History: A 42-year-old man presents with 9 months of epigastric pain.
1. Which of the following describes the abnormalities shown in the images? (Choose all that apply.)
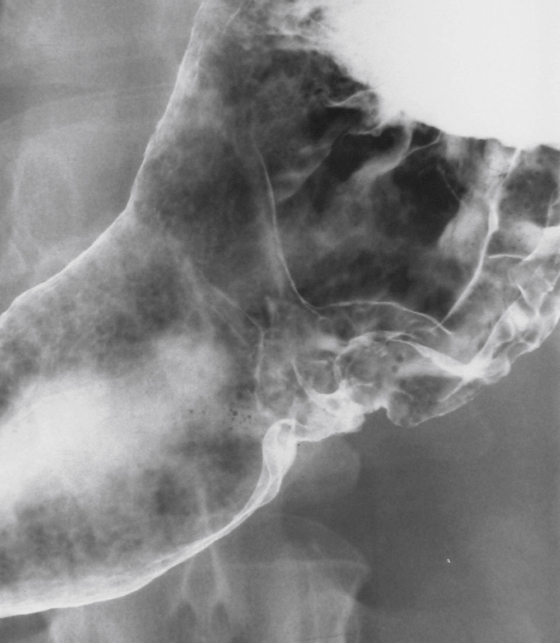
A. Ulcer along the greater curvature
C. Ulcer projects into the gastric lumen
D. Ulcer edge ragged and heaped up
E. Clubbed surrounding rugal folds
2. Which of the following features of a gastric ulcer is most suspicious for a malignant ulcer?
A. Ulcer is located in the gastric antrum.
B. Ulcer projects outside the gastric lumen.
C. There are clubbed surrounding rugal folds.
D. There is an associated duodenal ulcer.
E. Hampton’s line is apparent.
3. Which of the following does not have an association with gastric malignancy?
C. Helicobacter pylori infection
4. Of the following imaging modalities, which provides the best assessment of gastric cancer staging?
B. Barium upper GI study and follow-through
E. Endoscopic ultrasound (EUS)
ANSWERS
CASE 9
Malignant Ulcer of the Stomach
1. A, B, C, and D
2. C
3. B
4. C
References
Iyer R, Dubrow R. Imaging upper gastrointestinal malignancy. Semin Roentgenol. 2006;41(2):105–112.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 82-85.
Comment
Today, potential gastric malignancy is almost exclusively evaluated by endoscopy and CT. However in asymptomatic screening situations, high-quality double-contrast barium studies are still quite useful. Superficial spreading mucosal lesions with little or no mass can be missed on CT. Lesions such as those shown in the images from an upper GI study included with this case (see figures) are best augmented with CT evaluation, which allows much more accurate grading of the lesions. Perigastric involvement as well as lymph node spread and metastatic spread are well evaluated on multidetector computed tomography (MDCT) of the thorax, abdomen, and pelvis.
Some of the characteristics of benign gastric ulcer include the following:
• Hampton’s line, a well-defined thin lucency seen at the base of the ulcer, an ulcer collar






