CASE 88
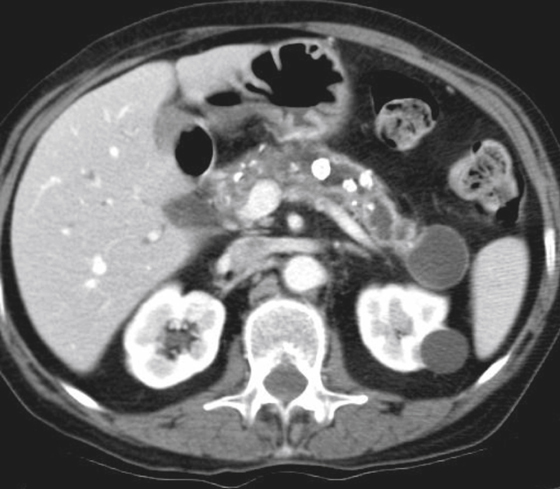
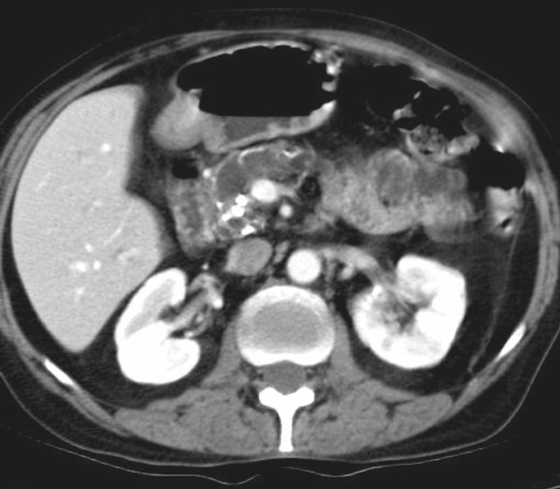
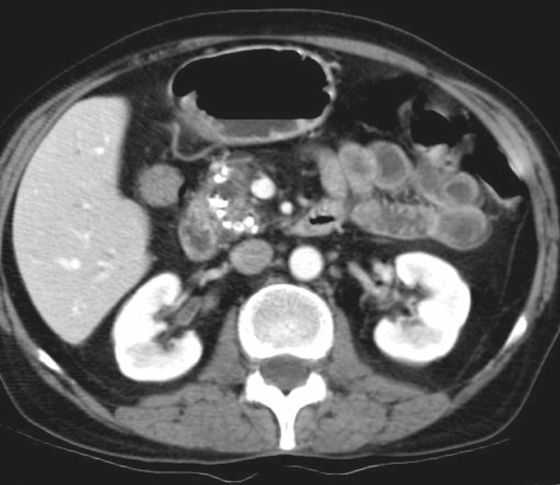
History: A 29-year-old man with chronic pancreatitis for 8 years presents with obstructive jaundice.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
B. Chronic pancreatitis stricture
C. Cancer of the pancreatic head
D. Calculus impacted at the ampulla
E. Intraductal papillary mucinous tumor
2. Which of the following statements regarding complications of chronic pancreatitis is true?
A. The cardinal symptom is abdominal pain.
B. Malabsorption occurs early in the course of the disease.
C. Endocrine insufficiency is usually mild, manifesting as non–insulin-dependent diabetes.
3. Which of the following statements regarding investigation of chronic pancreatitis is true?
A. Glandular calcification is radiographically visible in about 5% of patients.
B. Serum amylase and lipase levels are in a constant state of mild elevation.
C. MRI shows generalized increase in glandular signal owing to fatty replacement.
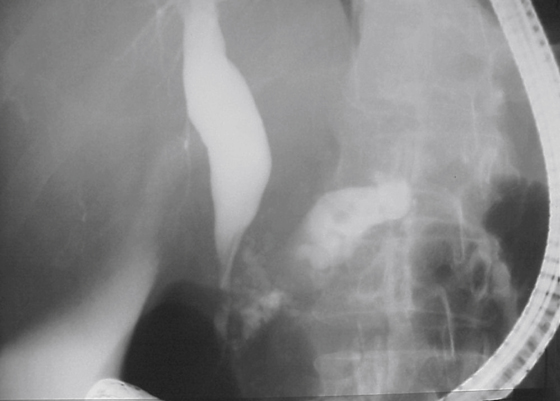
4. What is the double duct sign?
A. Dilation of the common bile and pancreatic ducts
B. Double pancreatic duct due to ectopic pancreatic rest
C. Endoscopic observation of double ducts draining the pancreas
D. Sonographic appearance of paired tubular anechoic structures in the liver
ANSWERS
CASE 88
Benign Stricture of Chronic Pancreatitis
1. B, C, and D
2. A
3. D
4. A
References
Remer EM, Baker ME. Imaging of chronic pancreatitis. Radiol Clin North Am. 2002;40:1229–1242.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 227.
Comment
Unlike stone formation in the bile duct, pancreatic stones (which usually form in the pancreatic ductal system rather than the acinar tissue) are not a major factor in pancreatic duct obstruction. In cases of benign stricture of the pancreas, the cause is usually chronic pancreatitis (see figures). When the stricture is located directly over the spine and there has been a prior history of blunt trauma to the abdomen, trauma should be included in the etiologic considerations.
Pancreatic strictures present a difficult therapeutic problem. The surgical approach, which includes the Puestow procedure (longitudinal pancreaticojejunostomy) and the Whipple procedure, involves long and highly invasive surgery, especially if there is no demonstrable mass on imaging. In recent years, placement of stents across a benign pancreatic duct has become more common, but there are problems associated with this as well. Although there have been reports of pain relief with stent placement, there is a question of whether a chronically dilated pancreatic duct can provide intrinsic drainage despite surgical intervention or stent placement. Moreover, pancreatic duct stents have an increased incidence of occlusion and are suspected by many investigators of causing chronic pancreatitis by their presence.






