[level-membership-for-gastroenterology-and-hepatology-category]CASE 86
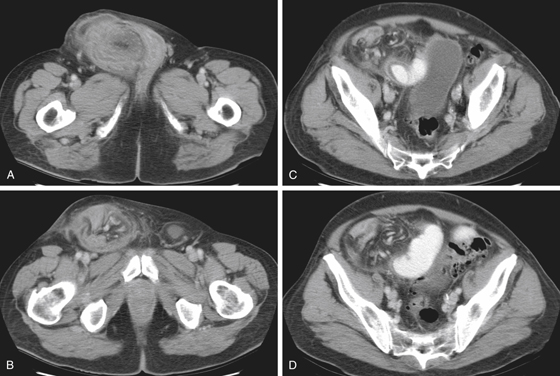
History: A 77-year-old man presents with abdominal pain and distention and vomiting.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. Which of the following statements about inguinal herniation is true?
A. The most common tumor of the inguinal canal is a lipoma.
B. Littre’s hernia is an inguinal hernia containing the vermiform appendix.
C. Inguinal herniation of the ovary typically occurs in post-menopausal women.
D. The most common primary site of metastases to the inguinal canal is melanoma from the skin.
3. What is the most common cause of small bowel obstruction?
4. What is the optimal method for demonstrating mechanical small bowel obstruction?
ANSWERS
CASE 86
Inguinal Hernia
1. A, B, D, and E
2. A
3. D
4. D
References
Aguirre DA, Santosa AC, Casola G, Sirlin CB. Abdominal wall hernias: imaging features, complications, and diagnostic pitfalls at multi-detector row CT. Radiographics. 2005;25:1501–1520.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 314.
Comment
Although the main cause of small bowel obstruction is surgical adhesions, hernias are another important cause, either in the abdominal wall or internally. Inguinal hernias are very common. Only ventral hernias are seen with more frequency. Both can lead to obstructive pathology, with inguinal hernia being more likely to incarcerate and obstruct as well as threaten the bowel’s blood supply (strangulated bowel).
For decades, contrast examination of the small bowel, along with plain film radiography, has been the standard for evaluating the patient with suspected obstruction. Enteroclysis or a dedicated small bowel follow-through have been shown to be of benefit, but they are often impractical for the postoperative patient, are time consuming, and are very uncomfortable for patients. Most now advocate the use of CT, which can assess the site of obstruction and possible underlying causes of the problem. It is as sensitive as the other modalities and can be quite specific for determining the cause of the problem, which is most helpful for clinicians (see figures).
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 86
History: A 77-year-old man presents with abdominal pain and distention and vomiting.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. Which of the following statements about inguinal herniation is true?
A. The most common tumor of the inguinal canal is a lipoma.
B. Littre’s hernia is an inguinal hernia containing the vermiform appendix.
C. Inguinal herniation of the ovary typically occurs in post-menopausal women.
D. The most common primary site of metastases to the inguinal canal is melanoma from the skin.
[/not-level-membership-for-gastroenterology-and-hepatology-category]
