CASE 85
History: A 32-year-old man with an abnormality noted on a routine chest x-ray.
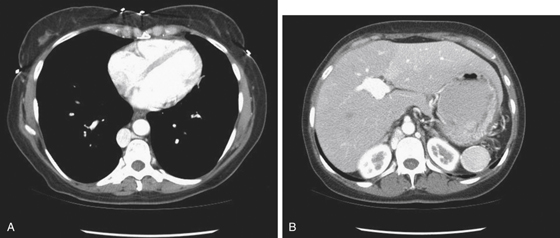
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
A. Azygous continuation of the inferior vena cava (IVC)
D. Obstruction of the superior vena cava
2. What is the physical cause of azygous continuation?
C. Lateral course of the azygous vein in a pleural septum
D. Occlusion, or failure of development of the IVC
3. Which of the following statements regarding azygous continuation is true?
C. Müller’s maneuver would cause the enlarged azygous vein to decrease in size.
D. This can be a congenital anomaly.
4. Which of the following is not a clinical significance of azygous continuation?
A. It may be mistaken for a mediastinal mass.
B. The patient is at risk for paradoxical embolism.
C. It is relevant in being able to undertake vascular procedures.
D. It alerts to the presence of other significant congenital disorders.
ANSWERS
CASE 85
Azygous Continuation
1. A, B, C, and D
2. D
3. D
4. B
References
Bass JE, Redwine MD, Kramer LA, et al: Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics. 2000;20:639–652.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 183.
Comment
Azygous continuation can be seen in a variety of settings. It can be a congenital failure of the development of the inferior vena cava or it can be chronic disease that slowly occludes the hepatic vein or the IVC over time. Any condition that results in hepatic venous occlusion can result in hepatomegaly and, if chronic, distention of the azygous-hemiazygous system as an alternative collateral route to return venous blood from the lower body to the heart. Such conditions include hepatoma and other indolent neoplasms as well as blood dyscrasias, such as sickle cell anemia and leukemia. In this case, the reason for the unusually large size of the azygous vein is failure of development of the IVC (see figures). Hepatic veins are visible but no IVC is identifiable (see figures). The finding was incidental. Other incidental CT findings in this vein would include duplication of the IVC, persistent cardinal vein, and commonly retroaortic left renal vein.






