CASE 85
History: No patient history is available.
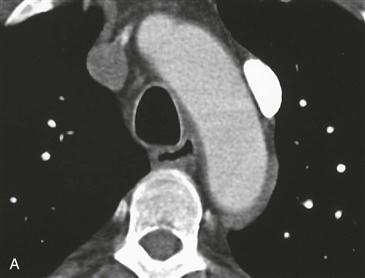
1. What should be included in the differential diagnosis of the vessel to the left of the aortic arch in Fig. A? (Choose all that apply.)
C. Persistent left superior vena cava (SVC)
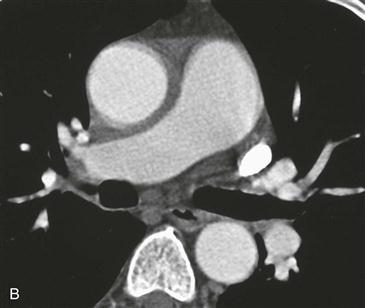
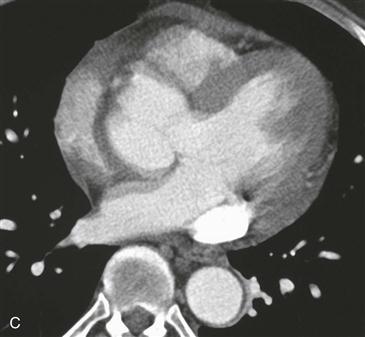
2. Taking into account all the figures, what is the most likely diagnosis?
3. What structure most commonly connects the right SVC and left SVC?
D. Right atrium
4. Which other anomaly occurs in most patients with persistent left SVC?
ANSWERS
References
Burney K, Young H, Barnard SA, et al. CT appearances of congenital and acquired abnormalities of the superior vena cava. Clin Radiol. 2007;62(9):837–842.
Uçar O, Paşaoğlu L, Ciçekçioğlu H, et al. Persistent left superior vena cava with absent right superior vena cava: a case report and review of the literature. Cardiovasc J Afr. 2010;21(3):164–166.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 27–29.
Comment
Etiology
Persistent left SVC results when the left anterior cardinal vein persists after birth. The left brachiocephalic vein drains into the left SVC, which usually connects to the coronary sinus. The coronary sinus may be dilated from the increase in flow, especially if there is no right SVC. Most individuals are asymptomatic, and their anatomy is otherwise normal. Most individuals with a persistent left SVC have a right SVC as well—hence the designation “duplicated SVC.”
Associated Anomalies
Rarely, the left SVC drains into the left atrium. In this situation, multiple severe cardiac anomalies may coexist, such as common atrium, atrioventricular canal defect, single ventricle, asplenia, and polysplenia. Persistent left SVC is also associated with atrial septal defect, tetralogy of Fallot, and partial and total anomalous pulmonary venous connection.