Procedure 83 Darrach Procedure
 See Video 62: Darrach Procedure
See Video 62: Darrach Procedure
Indications




Examination/Imaging
Clinical Examination











Surgical Anatomy





Exposures
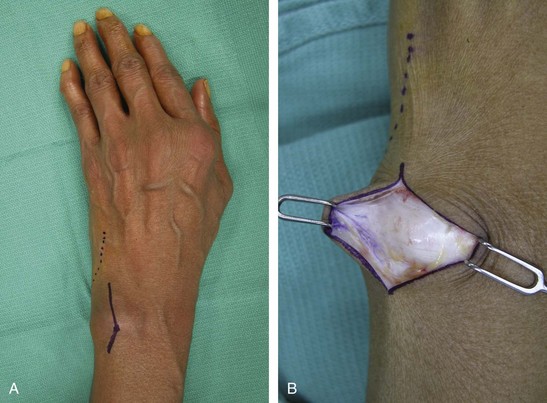
 A dorsal longitudinal incision over the distal ulna with a zigzag at the wrist is used for wide exposure to the level of the extensor retinaculum (Fig. 83-2A and B).
A dorsal longitudinal incision over the distal ulna with a zigzag at the wrist is used for wide exposure to the level of the extensor retinaculum (Fig. 83-2A and B).
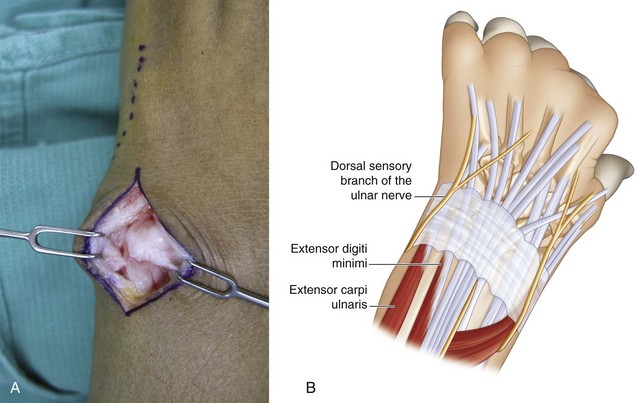
 Approach the ulna between the EDM and ECU and incise the periosteum to raise radial and ulnar periosteal flaps for later closure (Fig. 83-3A and B).
Approach the ulna between the EDM and ECU and incise the periosteum to raise radial and ulnar periosteal flaps for later closure (Fig. 83-3A and B).
Procedure
Step 1


Step 2




Step 3
 The dorsal wrist capsule is imbricated with 2-0 or 3-0 braided permanent horizontal mattress sutures with the wrist fully supinated, taking care to note that the ulna is not dorsally prominent in this position (Fig. 83-6). If the distal ulna stump is unstable with pronation-supination, an ulna-stabilizing procedure can be performed using a distally based ulnar half ECU tenodesis to correct prominence of the ulnar stump. This is performed as follows:
The dorsal wrist capsule is imbricated with 2-0 or 3-0 braided permanent horizontal mattress sutures with the wrist fully supinated, taking care to note that the ulna is not dorsally prominent in this position (Fig. 83-6). If the distal ulna stump is unstable with pronation-supination, an ulna-stabilizing procedure can be performed using a distally based ulnar half ECU tenodesis to correct prominence of the ulnar stump. This is performed as follows:
 The tourniquet is released, and all bleeding points are cauterized.
The tourniquet is released, and all bleeding points are cauterized.


Postoperative Care and Expected Outcomes



De Witte PB, Wijffels M, Jupiter JB, Ring D. The Darrach procedure for post-traumatic reconstruction. Acta Orthop Belg. 2009;75:316-322.
George MS, Kiefhaber TR, Stern PJ. The Sauve-Kapandji procedure and the Darrach procedure for distal radio-ulnar joint dysfunction after Colles’ fracture. J Hand Surg [Br]. 2004;29:608-613.
Minami A, Iwasaki N, Ishikawa J, et al. Treatments of osteoarthritis of the distal radioulnar joint: long-term results of three procedures. Hand Surg. 2005;10:243-248.

