CASE 82

History: A 54-year-old woman presents with abdominal distention.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
2. What is the original tumor described to cause pseudomyxoma peritonei?
3. Which of the following statements regarding pseudomyxoma peritonei is true?
A. The disease has equal sex distribution.
B. The most common presentation in women is increasing abdominal girth.
C. The most common presentation in men is the development of an inguinal hernia.
D. Disease tends to involve the peritoneal surfaces of the bowel.
4. What is the definitive treatment for pseudomyxoma peritonei?
ANSWERS
CASE 82
Pseudomyxoma Peritonei
1. A, B, and C
2. D
3. B
4. D
References
Levy AD, Shaw JC, Sobin LH. Secondary tumors and tumorlike lesions of the peritoneal cavity: imaging features with pathologic correlation. Radiographics. 2009;29:347–373.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 138.
Comment
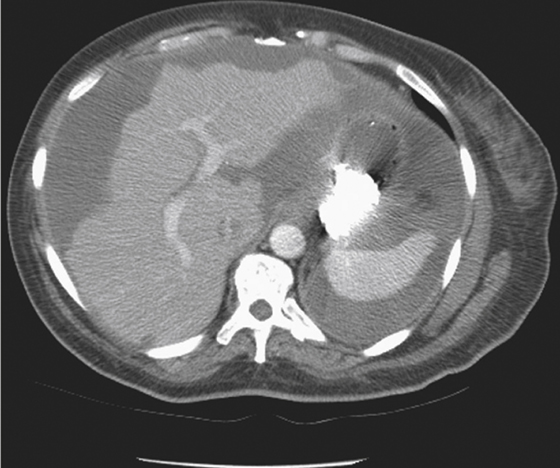
These CT images demonstrate large collections of low-density material throughout the abdominal cavity, resembling ascites. However, in this instance the material appears loculated or cystic in the lower abdominal cavity. Scalloping of the liver edge also is present. Finally, areas of fine calcification are evident within the peritoneal cavity on some of the images. All these findings make this case atypical for conventional ascites and suggest the possibility of pseudomyxoma peritonei.
Pseudomyxoma peritonei is the presence of gelatinous or mucinous material in the peritoneal cavity. It is produced by the rupture of a mucin-producing neoplasm into the peritoneal cavity. It can be either a malignant process, such as a mucinous adenocarcinoma, or a benign process, such as a mucocele of the appendix. Once the tumor ruptures, the cellular debris continues to produce mucin within the peritoneum, and the process tends to be progressive whether it is the result of a benign or a malignant cause.
In women by far the most common cause of pseudomyxoma peritonei is a mucinous neoplasm of the ovary, typically mucinous cystadenocarcinoma. In men the usual origin of the process is an appendiceal tumor, such as a mucocele of the appendix or a mucinous cystadenocarcinoma. Mucinous cystic tumors of the pancreas also can cause this condition. Mucinous tumors of the stomach, intestines, or bile ducts are even more rare. In this patient the scalloping of the liver and the calcification favor the diagnosis of a malignant mucinous process. Treatment is typically supportive because the material cannot be successfully removed surgically, and the remaining cells within the peritoneum will continue to produce the material.






