CASE 80


1. What should be included in the differential diagnosis for a left-to-right shunt? (Choose all that apply.)
A. Partial anomalous pulmonary venous return (PAPVR)
2. What is the cardiac finding?
A. ASD
3. What is the most likely cause of the right atrial and ventricular enlargement in this patient?
B. Primary pulmonary hypertension
4. What is the pulmonary finding?
ANSWERS
CASE 80
References
Hijii T, Fukushige J, Hara T. Diagnosis and management of partial anomalous pulmonary venous connection: a review of 28 pediatric cases. Cardiology. 1998;89(2):148–151.
Ho ML, Bhalla S, Bierhals A, et al. MDCT of partial anomalous pulmonary venous return (PAPVR) in adults. J Thorac Imaging. 2009;24(2):89–95.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 330–335.
Comment
Imaging
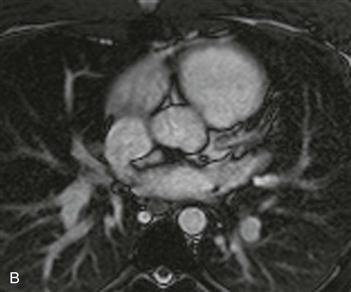
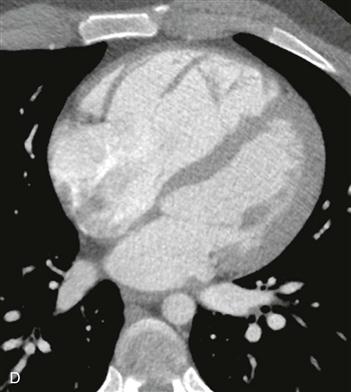
MRI shows anomalous drainage of a portion of the right lung into the superior vena cava (Fig. A). PAPVR is an atrial level shunt. Images of the heart (Figs. B and C) show a defect in the interatrial septum located posteriorly and superiorly, which is consistent with a sinus venosus ASD. This patient had a large left-to-right shunt (Fig. D) and underwent surgical correction with ASD patching and redirection of the anomalous pulmonary veins into the left circulation.
Associations
PAPVR may be associated with other congenital abnormalities, most commonly a sinus venosus ASD (sinus venosus defect). Patients can be asymptomatic but may present with dyspnea, exercise intolerance, pulmonary hypertension, or syncope depending on the degree of shunt. The indications for surgical correction are symptoms or a large shunt (i.e., pulmonary blood flow twice that of systemic blood flow). Magnetic resonance angiography (MRA) can accurately depict the presence, size, and location of the PAPVR and ASD. MRI can quantify the shunt fraction and help determine the ideal timing to perform surgery.






