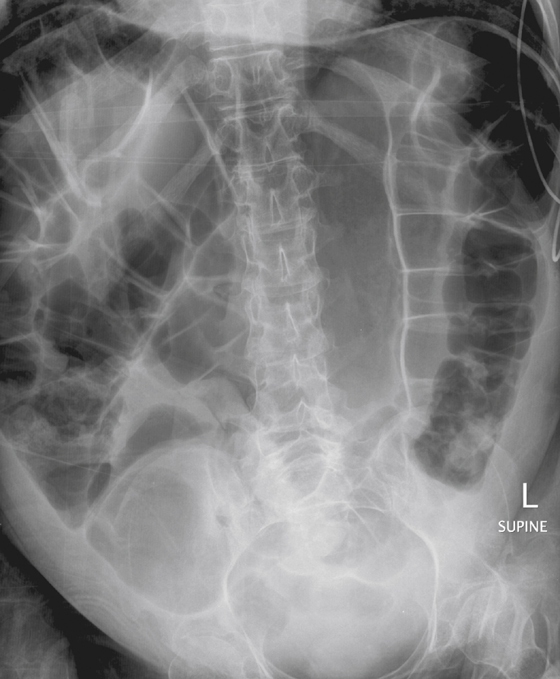
History: A 24-year-old man with muscular dystrophy developed acute abdominal distention 18 hours ago.
1. Which of the following should be included in the differential diagnosis for this patient? (Choose all that apply.)
E. Colonic ileus (Ogilvie syndrome)
2. What is the most common form of volvulus seen in the colon?
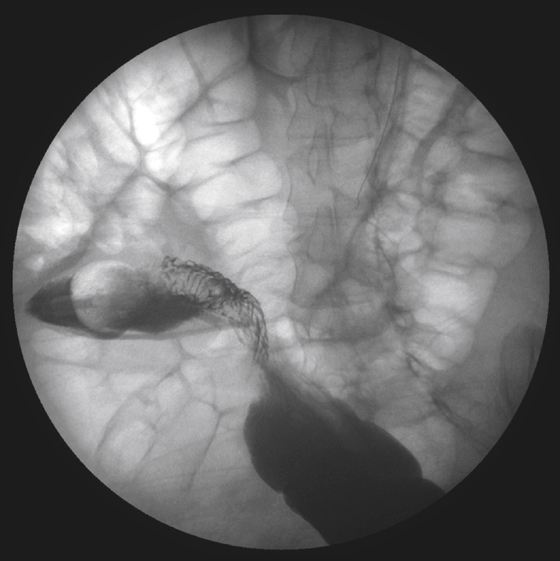
3. What is the name of the radiologic sign seen at the site of torsion on contrast enema?
4. All of the following statements about sigmoid volvulus are true except:
B. Laparotomy and sigmoidopexy are the therapy of choice.
C. A redundant sigmoid colon is a predisposing factor.
ANSWERS
CASE 8
Sigmoid Volvulus
1. D
2. A
3. B
4. B
References
Feldman D. The coffee bean sign. Radiology. 2000;216:178–179.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 310.
Comment
Sigmoid volvulus is the most common type of volvulus seen in the gastrointestinal tract, accounting for 8% to 10% of cases of large bowel obstruction. The incidence is higher in areas of the world where roundworm infestation is endemic. In the West, the condition tends to occur in older patients (slightly higher rate in men), with a mortality rate of about 20%. Ultimately the mortality rate depends upon the degree of torsion and the time between the onset of symptoms and diagnosis and treatment. The amount of torsion around the sigmoid mesentery can vary from 180 to 540 degrees and usually occurs about 20 to 25 cm from the anal verge. The torsion is counterclockwise. Patients commonly present with abdominal distention and pain and inability to pass stool or gas.
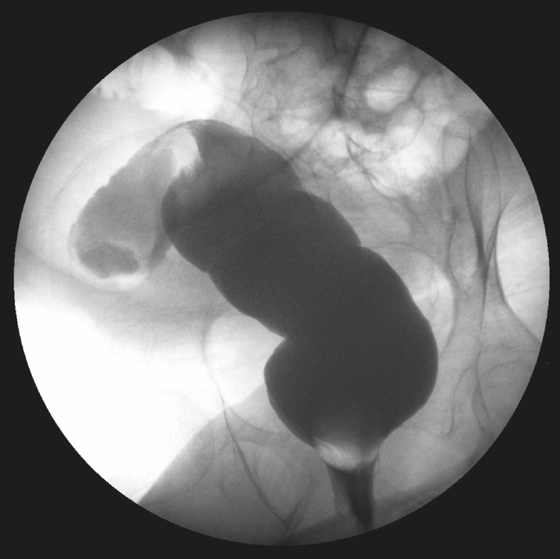
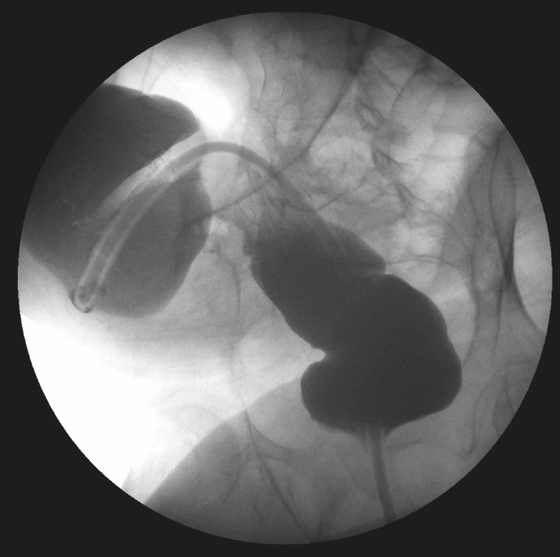
Plain films of the abdomen are often enough to make the diagnosis in 70% of patients (see figures). They show a grossly dilated sigmoid colon in the well-known coffee bean configuration arising out of the pelvis. The sigmoid haustra is effaced and there may be evidence of proximal obstruction if the amount of torsion is so great as to become an obstruction above the volvulus. Most of the time the torsion allows proximal air to pass into the volvulus but does not permit retrograde or distal escape of air, and evidence of proximal obstruction might not be present in such cases. If no free air is present and there is no evidence of pneumatosis or clinical evidence of peritonitis, a water-soluble enema is the best choice among contrast examinations. Contrast material will demonstrate a normal-caliber distal sigmoid and rectum, but will taper to the diagnostic bird beak sign at the site of torsion (see figures).






