CASE 8

History: No patient history is available.
1. What should be included in the differential diagnosis? (Choose all that apply.)
C. Descending thoracic aortic aneurysm
2. Which of the following conditions is most commonly associated with this lesion?
3. What sign or symptom is this patient most likely to have?
A. Hypertension
B. Chest pain
4. Which modality provides the most helpful information in diagnosing this condition?
B. MRI
C. CT
D. Scintigraphy
ANSWERS
Reference
Kimura-Hayama ET, Meléndez G, Mendizábal AL, et al. Uncommon congenital and acquired aortic diseases: role of multidetector CT angiography. Radiographics. 2010;30(1):79–98.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 419–424.
Comment
Epidemiology
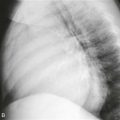
Aortic coarctation represents a discrete narrowing of the aorta and is usually juxtaductal in location when discovered later in life. Multiple signs on the chest radiograph may alert the radiologist to the presence of aortic coarctation. The “figure 3” sign represents an abnormal aortic contour with a sharp point occurring at the site of coarctation. This sign occurs in 60% of cases and is usually seen in patients with adult-type coarctation. An additional imaging sign is the presence of inferior rib notching. Rib notching occurs secondary to dilated intercostal arteries, which function as a collateral route for blood flow around the site of aortic narrowing. The main pathway of collateral flow proceeds as follows: aortic arch to subclavian artery to internal mammary artery to intercostal artery to descending thoracic aorta. Additional collateral pathways around the coarctation include the thyrocervical, thoracoacromial trunk, and epigastric arteries.
Associations
The most common association with coarctation is a bicuspid aortic valve followed by Turner syndrome. Aortic coarctation is frequently fatal if it is left untreated. Causes of death include congestive heart failure, aortic dissection, endocarditis, and aortic rupture. Patients are also predisposed to cerebral aneurysms with intracranial hemorrhage owing to carotid artery hypertension.
Imaging
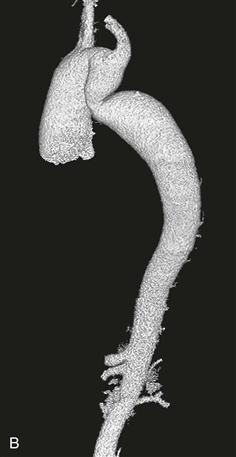
Chest radiography shows a mildly enlarged distal aortic arch that abruptly comes to a sharp point consistent with the “figure 3” sign of aortic coarctation (Fig. A). Volume-rendered CT angiography (Fig. B) also shows the typical “figure 3” sign. The narrowing is distal to the left subclavian artery.
Differential Diagnosis
The main differential diagnosis is aortic pseudocoarctation. MRI is helpful in distinguishing between these two conditions because pseudocoarctation is not associated with a pressure gradient or collateral flow around the narrowed segment.