[level-membership-for-gastroenterology-and-hepatology-category]CASE 79
History: An 86-year-old woman presents with nausea and vomiting for 2 weeks.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the most common cause of gastric outlet obstruction?
3. Which malignancy is most likely to cause gastric outlet obstruction?
4. Which of the following statements about gastric outlet obstruction is false?
A. A short history of symptoms is suspicious for malignancy.
B. The organoaxial type of gastric volvulus is more likely to cause gastric outlet obstruction.
C. Gastric outlet obstruction is the most common complication of gastroduodenal tuberculosis.
D. Gastric outlet obstruction can occur as a complication of percutaneous gastrostomy tube migration
ANSWERS
CASE 79
Gastric Outlet Obstruction
1. A, B, D, and E
2. D
3. C
4. B
Reference
Eisenberg RL, Levine MS. Miscellaneous abnormalities of the stomach and duodenum. In: Gore RM, Levine MS, eds. Textbook of Gastrointestinal Radiology. 2nd ed Philadelphia: WB Saunders; 2000:659–681.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 49.
Comment
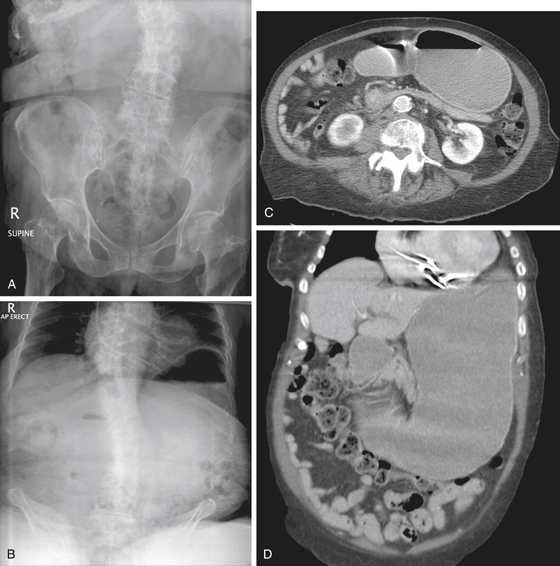
With newer and more-effective medications inhibiting acid secretion, gastric outlet obstruction is not as common as it was 20 years ago. However, peptic ulcer disease (PUD) is still the most common cause. Malignancy is becoming a larger and more dangerous issue as a cause for gastric outlet obstruction in the 21st century. Patients who have a long history of PUD and who have ineffective treatment or do not comply with the medication regimen (e.g., alcoholics) and who present with pain and gastric distention probably have ulceration and inflammation as the cause of their obstruction. Alternatively, severe pancreatitis that causes inflammation and spasm of the second portion of the duodenum can also obstruct the gastric outlet. In patients who have little or no history of PUD and who present with gastric outlet obstruction, the possibilities are more ominous, such as carcinoma of the distal antrum or pylorus, as well as pancreatic carcinoma invading and obstructing the duodenum. In this case, pancreatic cancer with duodenal invasion was the cause of the outlet obstruction (see figures).
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 79
History: An 86-year-old woman presents with nausea and vomiting for 2 weeks.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the most common cause of gastric outlet obstruction?
3. Which malignancy is most likely to cause gastric outlet obstruction?
[/not-level-membership-for-gastroenterology-and-hepatology-category]
