CASE 78

History: A 27-year-old man has a long history of constipation dating back to his infancy.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
2. What is the pathologic basis of Hirschsprung’s disease?
A. A segment of colonic aperistalsis
B. A segment of submucosal fibrosis
C. A segment of persistent contraction of intramural smooth muscle
D. A segment of congenitally absent ganglion cells in the distal colon
3. What other conditions is most commonly seen with Hirschsprung’s disease?
4. Which of the following statements about Hirschsprung’s disease is true?
A. The disease is more common in girls than boys.
B. In about 5% of cases, the entire colon is involved.
C. Treatment of choice is dilatation of the narrow segment.
D. Barium enema and rectal manometry are the optimal diagnostic tools.
ANSWERS
CASE 78
Adult Hirschsprung’s Disease
1. A, C, D, and E
2. D
3. D
4. B
References
Crocker NL, Messmer JM. Adult Hirschsprung’s disease. Clin Radiol. 1991;44:257–259.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 304.
Comment
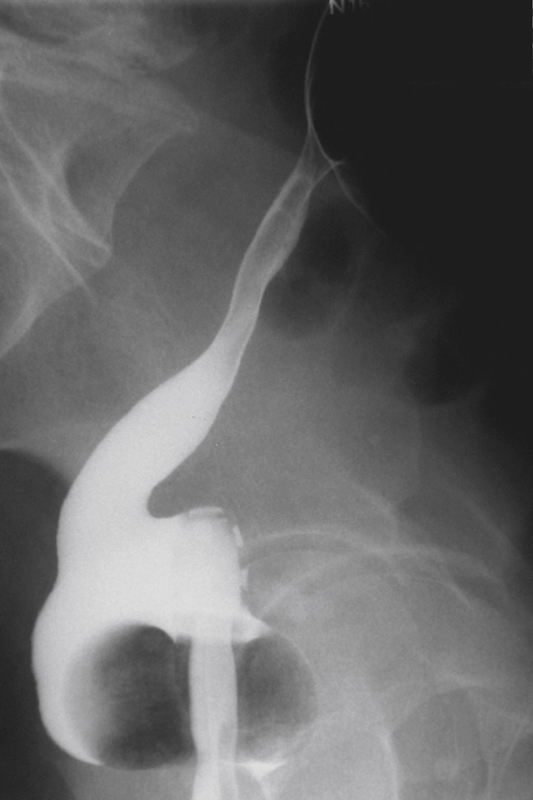
Hirschsprung’s disease is named after Harald Hirschsprung, the Danish physician who described the disease in 1888. It is a congenital disorder of the gut characterized by a segment of absent ganglion cells in the distal colon. The degree of involvement can vary, but most cases are diagnosed in the neonatal stage with the failure to pass meconium. However, lesser degrees of aganglionosis can result in a delayed diagnosis. The massive enlargement of the colon is obvious. The aganglionic segment is also visible in the rectum. The disease is more common in boys and has no racial predilection. Patients who have delayed diagnosis are much affected by the disease. They suffer from chronic severe debilitating constipation, abdominal distention, some with encopresis and an overall life-altering health state.
Plain films are suggestive in most cases. CT may be diagnostic, showing the classic features recognized by barium enema of a narrowed distal colon with proximal dilation (see figures). Barium enema has the benefit of acquiring a 24-hour-delayed radiograph that will show retention of the contrast. Rectal biopsy is the definitive diagnostic procedure. Surgery aimed at the removal of the aganglionic segment and some excess colon is usually the treatment of choice. Laparoscopic surgery for Hirschsprung’s disease in newborns has been reported with some initial success.






