Procedure 77 Volar Plating of Distal Radius Fractures
 See Video 58: Volar Locking Plate Fixation for Distal Radius Fractures
See Video 58: Volar Locking Plate Fixation for Distal Radius Fractures








Surgical Anatomy





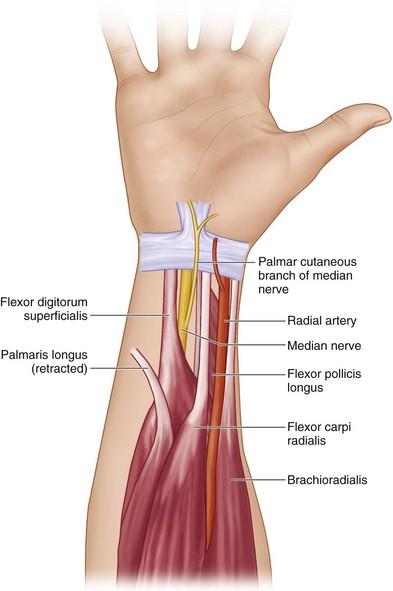

Exposures
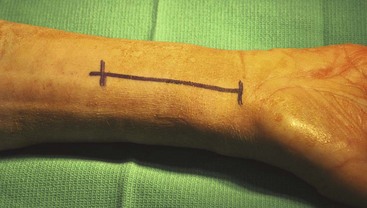
 An incision about 7 cm in length is made over the forearm between the radial artery and the FCR. The distal aspect of the incision stops at the volar wrist crease (Fig. 77-3). If the incision needs to be extended more distally, a V-shaped zigzag extension should be made.
An incision about 7 cm in length is made over the forearm between the radial artery and the FCR. The distal aspect of the incision stops at the volar wrist crease (Fig. 77-3). If the incision needs to be extended more distally, a V-shaped zigzag extension should be made.
 The FCR tendon is exposed and released from its sheath. The dissection should remain on the radial aspect of the FCR (Fig. 77-4).
The FCR tendon is exposed and released from its sheath. The dissection should remain on the radial aspect of the FCR (Fig. 77-4).
 The radial artery and its accompanying venae comitantes are exposed and retracted radially. All ulnar crossing vessels are coagulated (Fig. 77-5).
The radial artery and its accompanying venae comitantes are exposed and retracted radially. All ulnar crossing vessels are coagulated (Fig. 77-5).
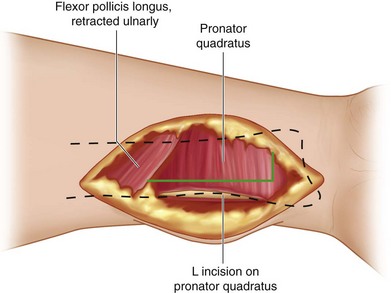
 The PQ is elevated from the distal radius by making an L-shaped incision and releasing it radially and distally (Fig. 77-6). The PQ is sharply released from the radius to expose the fracture (Fig. 77-7).
The PQ is elevated from the distal radius by making an L-shaped incision and releasing it radially and distally (Fig. 77-6). The PQ is sharply released from the radius to expose the fracture (Fig. 77-7).



Pearls
It is helpful to mobilize the radial artery and ligate its small crossing branches during the exposure. This minimizes bleeding and also allows for better exposure of the BR for release.
Do not take the reflection of the soft tissue too far distally on the radius. This may result in release of the volar carpal ligaments from the distal radius and induce carpal instability.
Procedure
Step 1
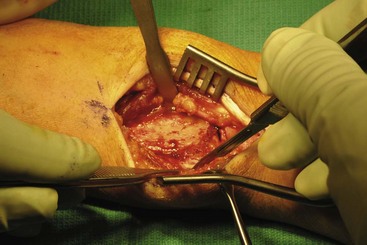
 The volar radius is exposed, and the distal fragment is exposed by releasing the BR tendon. The distal fragment is usually displaced dorsally (Fig. 77-8).
The volar radius is exposed, and the distal fragment is exposed by releasing the BR tendon. The distal fragment is usually displaced dorsally (Fig. 77-8).
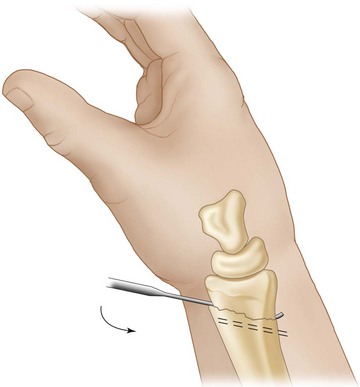
 A Freer elevator may be used to lever the distal fragment for fracture reduction (Fig. 77-9). The elevator should be inserted to the dorsal cortex to completely disimpact the distal fragment to aid in reduction.
A Freer elevator may be used to lever the distal fragment for fracture reduction (Fig. 77-9). The elevator should be inserted to the dorsal cortex to completely disimpact the distal fragment to aid in reduction.

Step 2
 The reduced fracture may be provisionally held with K-wires placed through the open approach or through a small separate radial styloid incision (Fig. 77-10).
The reduced fracture may be provisionally held with K-wires placed through the open approach or through a small separate radial styloid incision (Fig. 77-10).
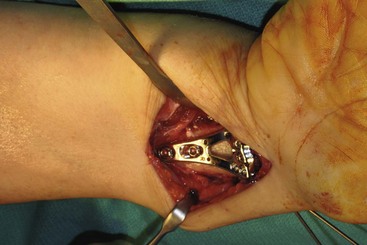
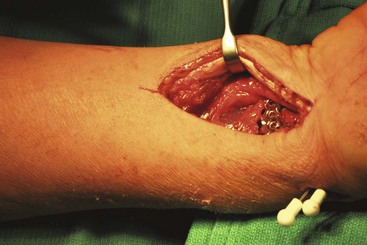
 The plate is placed centrally on the radial shaft and as far distally as necessary to capture the distal fragment. It is crucial to be familiar with the specific plate distal locking screw trajectory for proper plate placement (Fig. 77-11).
The plate is placed centrally on the radial shaft and as far distally as necessary to capture the distal fragment. It is crucial to be familiar with the specific plate distal locking screw trajectory for proper plate placement (Fig. 77-11).
 The volar plate is then applied to the radial shaft, and a screw is inserted first in the elongated elliptical hole. A 2.0-mm drill bit is drilled in the center of the hole, and a 2.7-mm screw is then placed (Fig. 77-12).
The volar plate is then applied to the radial shaft, and a screw is inserted first in the elongated elliptical hole. A 2.0-mm drill bit is drilled in the center of the hole, and a 2.7-mm screw is then placed (Fig. 77-12).





Step 3
 The distal screws are next placed in the plate with the wrist in a flexed position. These screws are 2.4 mm in size and are drilled with a 1.8-mm drill bit. If the fracture is properly reduced, a locking screw may be placed (Fig. 77-13).
The distal screws are next placed in the plate with the wrist in a flexed position. These screws are 2.4 mm in size and are drilled with a 1.8-mm drill bit. If the fracture is properly reduced, a locking screw may be placed (Fig. 77-13).

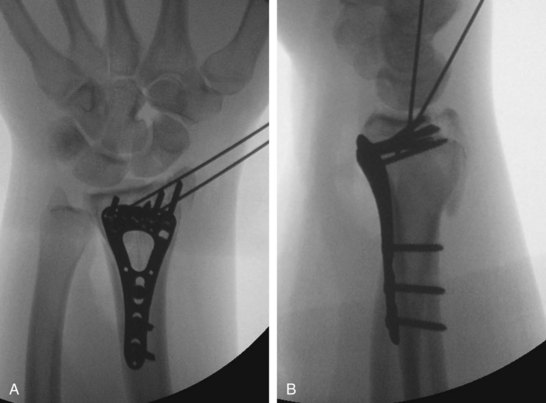
 A sufficient number of screws should be placed in the distal aspect of the plate to ensure adequate purchase of all the fracture fragments (Fig. 77-14).
A sufficient number of screws should be placed in the distal aspect of the plate to ensure adequate purchase of all the fracture fragments (Fig. 77-14).

Step 3 Pearls
A fossa lateral view of the distal radius should be taken to ensure no joint penetration of the screws. A fossa lateral view is taken by holding the forearm at about 22 degrees of inclination with regard to the hand table. This corrects the overlap of the articular surface caused by the radial inclination on a standard lateral view (Fig. 77-15).
The designed purpose of the distal screw row is for subchondral support, whereas the proximal screw row provides distal-dorsal fixation.

Step 4
 The PQ is replaced over the plate and sutured to its radial attachment and periosteum (Fig. 77-16).
The PQ is replaced over the plate and sutured to its radial attachment and periosteum (Fig. 77-16).
 The wound is closed with 3-0 Vicryl sutures in the subcutaneous tissue and interrupted 3-0 nylon sutures in the skin (Fig. 77-17).
The wound is closed with 3-0 Vicryl sutures in the subcutaneous tissue and interrupted 3-0 nylon sutures in the skin (Fig. 77-17).
 The patient is placed in a short-arm volar splint at the end of the surgical procedure.
The patient is placed in a short-arm volar splint at the end of the surgical procedure.

Postoperative Care and Expected Outcomes





Orbay J, Badia A, Khoury RK, et al. Volar fixed-angle fixation of distal radius fractures: the DVR plate. Tech Hand Up Extrem Surg. 2004;8:142-148.
Orbay JL, Fernandez DL. Volar fixed-angle plate fixation for unstable distal radius fractures in the elderly patient. J Hand Surg [Am]. 2004;29:96-102.
Rizzo M, Katt BA, Carothers JT. Comparison of locked volar plating versus pinning and external fixation in the treatment of unstable intraarticular distal radius fractures. Hand. 2008;3:111-117.
Souer JS, Ring D, Matschke S, et al. Comparison of functional outcome after volar plate fixation with 2.4-mm titanium versus 3.5-mm stainless-steel plate for extra-articular fracture of distal radius. J Hand Surg [Am]. 2010;35:398-405.
Wei DH, Raizman NM, Bottino CJ, et al. Unstable distal radial fractures treated with external fixation, a radial column plate, or a volar plate: a prospective randomized trial. J Bone Joint Surg [Am]. 2009;91:1568-1577.


