[level-membership-for-gastroenterology-and-hepatology-category]CASE 77
History: A 41-year-old woman presents with recurrent dyspepsia despite H2 blocker treatment.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
2. What is the leading cause of gastroduodenal ulcer disease in industrialized societies?
3. What substance does the breath test for gastric H. pylori infection in the upper gastrointestinal tract detect?
4. What is the treatment of choice for this infection?
ANSWERS
CASE 77
Helicobacter Gastritis
1. B, C, D, and E
2. D
3. D
4. C
References
Levine MS. Inflammatory conditions of the stomach and duodenum. In: Gore RM, Levine MS, eds. Textbook of Gastrointestinal Radiology. 2nd ed Philadelphia: WB Saunders; 2000:546–574.
Nadgir RN, Levine MS. Update on Helicobacter pylori. Appl Radiol. 1999;28:10–14.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 66.
Comment
The presence of H. pylori in the upper gastrointestinal tract is now believed to be the major cause of peptic ulcer disease among persons who live in industrialized countries. The majority of gastric ulcers also are attributed to this organism, which is considered a major cause of chronic gastritis as well. Almost all duodenal ulcer patients also have H. pylori infection.
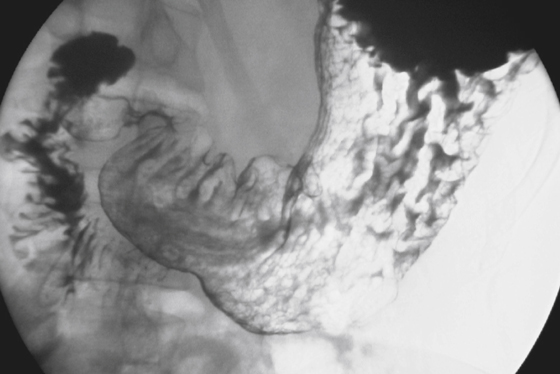
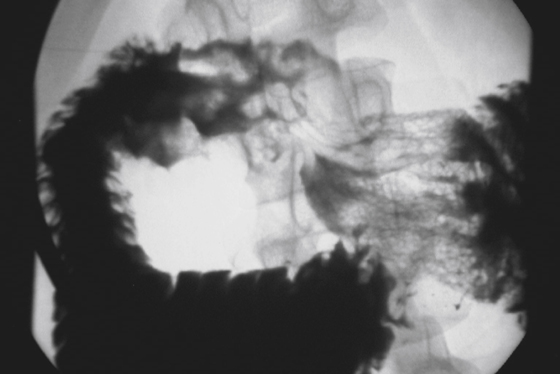
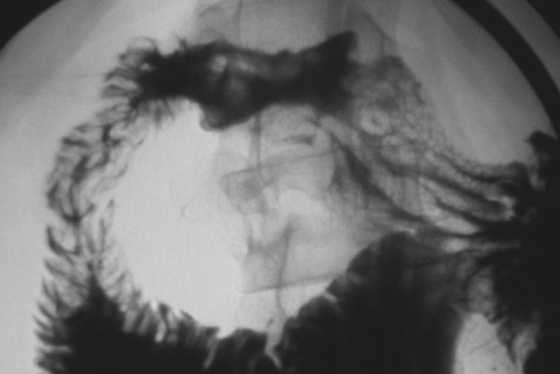
The radiologic abnormalities in these patients can be quite variable, and many patients have normal radiologic studies. By far the most common radiologic abnormality seen in patients with H. pylori infection is thickened gastric folds (see figures). The abnormality can vary from mild thickening of the folds in either the proximal stomach or antral region to bizarrely nodular folds involving a large portion of the stomach. These folds can become so thickened that they resemble a neoplastic process, such as lymphoma. Often these fold abnormalities can be detected on CT examination. Polyps of varying sizes also have been described. Typically these are small hyperplastic polyps, although rarely a large focal polypoid mass is encountered. In many of these patients, endoscopy is necessary to exclude malignancy. Of course, ulcers and erosions can be identified in the stomach, but this finding is less common than are the fold abnormalities. Enlarged areae gastricae also have been described, although this finding is subtle. In the duodenum, radiologic findings include ulcers, thickened folds, and narrowing or deformity.
Noninvasive techniques for detecting H. pylori include a breath test that detects urease activity within the upper gastrointestinal tract. Serologic tests can detect antibodies to the H. pylori antigen. Endoscopic studies are considered the mainstay for detection because the bacteria can be identified on biopsy specimens. However, the infection itself is patchy, and multiple biopsies are often necessary to detect the organism.
Treatment includes antibiotic therapy, usually involving a combination of agents, including metronidazole, tetracycline, or amoxicillin. Oral bismuth therapy is also recommended, and histamine blockers or proton-pump inhibitors are given to reduce acid levels.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 77
History: A 41-year-old woman presents with recurrent dyspepsia despite H2 blocker treatment.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
2. What is the leading cause of gastroduodenal ulcer disease in industrialized societies?
3. What substance does the breath test for gastric H. pylori infection in the upper gastrointestinal tract detect?
[/not-level-membership-for-gastroenterology-and-hepatology-category]
